Disproportionate Share Hospital Programs |
|
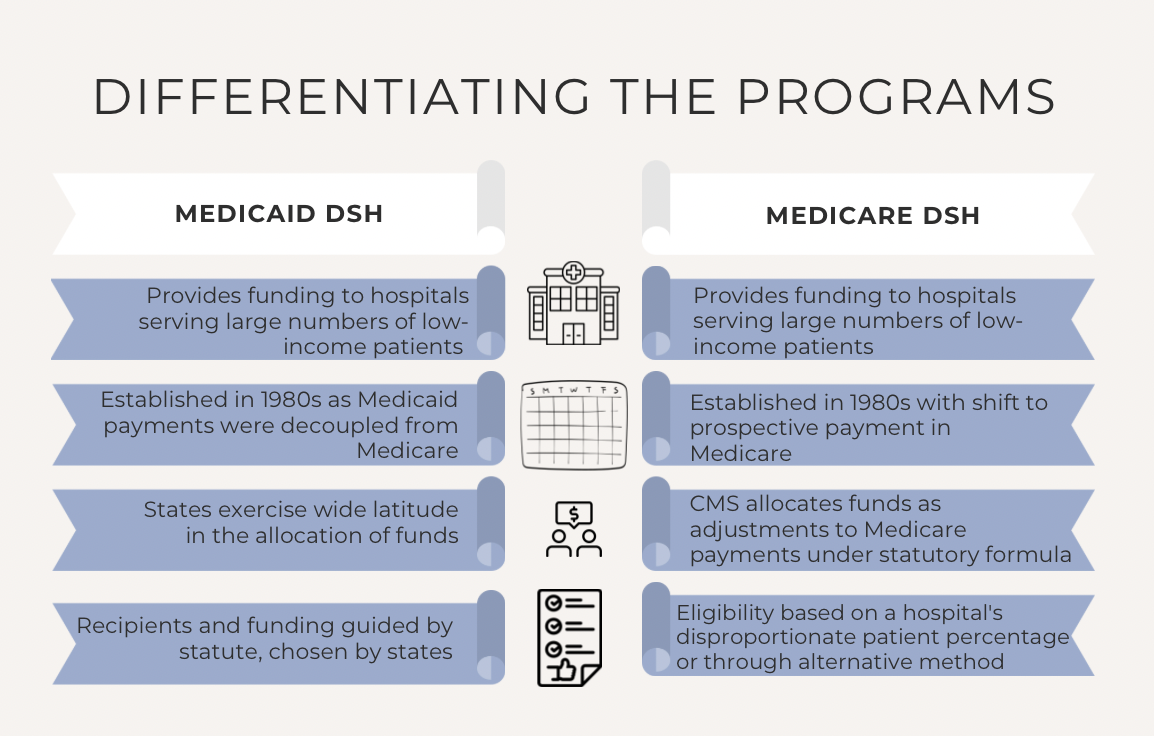
The Medicaid and Medicare Disproportionate Share Hospital (DSH) programs share a common goal of providing support to hospitals serving large numbers of low-income patients. Yet, despite this shared purpose, the two programs differ significantly in terms of operational frameworks, eligibility criteria, and policy issues. In our featured articles this month, we examine each program in detail. |
|
The Medicaid DSH program is an important component of the United States' broader effort to provide healthcare to its most disadvantaged citizens. Initiated to offset the financial burdens faced by hospitals delivering care to uninsured and low-income patients, Medicaid DSH payments have become a cornerstone of funding for many safety-net hospitals.
However, while well-intentioned, the Medicaid DSH program has faced scrutiny over its methodologies and effectiveness. Critics have previously raised concerns about the program's operational strategies and cost effectiveness. Now, some are even questioning if this program, upon which many essential hospitals rely, aligns with contemporary standards of health equity.
|
|
True or False?
Both the Medicaid and Medicare DSH programs
specifically employ the designation of "Pickle" hospitals.
(Find the answer at the bottom of the page.*)
|
|
The impetus for the establishment of the Medicare DSH program, like that of Medicaid DSH, can be traced to significant changes in the Medicare payment model undertaken in the 1980s.
Medicare’s transition from a reasonable-cost reimbursement system to a prospective payment system (PPS) required that Congress consider how the new payment model would impact the financial stability of certain hospitals, particularly those serving a high volume of low-income patients. The Medicare DSH program was established as a way to quantify and mitigate these hospitals' financial losses.
In the decades since the program’s inception, Medicare DSH payment adjustments have become critical to the financial health of qualifying hospitals. But even Supreme Court justices have found themselves puzzling over what the Centers for Medicare & Medicaid Services (CMS) acknowledges is a "complex formula" for determining payments.
|
|
AI HealthWatch: Navigating Federal Policies |
|
In our commitment to keeping our readers at the forefront of healthcare policy and innovation, Applied Policy Insight is pleased to introduce a new, regular feature: an in-depth exploration of policies specific to the use of artificial intelligence (AI) in healthcare.
This new column from Will Henkes, Health Policy Associate, is envisioned as a go-to source for understanding how directives from the Department of Health and Human Services (HHS) and other federal agencies are shaping the use of AI in the healthcare sector.
While policy will be our guiding star, Will will also occasionally delve into the latest AI technologies and innovations that are set to impact healthcare delivery and management.
In his inaugural column, Will considers reimbursement strategies for AI.
|
|
AI Reimbursement Lags Technology |
|
Under the inpatient prospective payment system (IPPS), firms that own new and expensive technologies can apply for these technologies to receive new technology add-on payments (NTAPs.) The NTAP program was created in 2001 after Congress, concerned that the existing IPPS reimbursement structure did not incentivize the use of new technologies, passed a law requiring CMS to design a mechanism to recognize the cost of new medical services and technologies under the IPPS. NTAP applicants must prove that their technology is new, costly, and provides substantial clinical improvements. If the technology has been designated as a breakthrough device by the Food and Drug Administration (FDA), CMS assumes that this technology is new and provides substantial clinical improvements, and the applicant must only meet the cost criterion. All applicants must receive FDA approval by May 1 prior to the fiscal year for which they are applying for NTAP designation. Once a product has been designated for NTAP, hospitals utilizing this product receive an add-on payment outside of the standard IPPS Medicare Severity Diagnosis-Related Group (MS-DRG) payment amount. This add-on payment is equal to 65 percent of the difference between the cost of the case utilizing the technology and the standard MS-DRG payment, capped at 65 percent of the cost of the technology. NTAP designation cannot last more than three years.
As AI has become more prevalent in healthcare, and as the benefits of the technology become more apparent, policymakers have been forced to consider how these technologies can be reimbursed under Medicare. As no dedicated reimbursement mechanism exists for AI in Medicare, NTAP has become the default way to reimburse for these technologies under the IPPS. However, the uptake of AI in healthcare has far exceeded the rate at which these products are approved for NTAP reimbursement.
|
|
Applied Policy's Latest Summaries |
|
CMS Proposes FY 2025 Inpatient Payment Policies for Hospitals and New Mandatory Payment Model (CMS-1808-P) |
|
On April 10, CMS issued the fiscal year (FY) 2025 Hospital Inpatient Prospective Payment Systems (IPPS) for Acute Care Hospitals and the Long-Term Care Hospital (LTCH) Prospective Payment System proposed rule.
The rule proposes to:
- Increase hospital operating payment rates by 2.6 percent,
- Continue the hospital low wage index policy and update labor market areas,
- Continue to calculate disproportionate share hospital payments from three years of uncompensated care data,
- Change the severity designation of inadequate housing and housing instability Z codes,
- Make changes to criteria for new residency programs and distribute 200 additional residency slots as required by the Consolidated Appropriations Act, 2023.
|
|
CMS Finalizes CY 2025 Policy Changes for Medicare Advantage and Part D Plans Impacting Patient Protections, Utilization Management, and Formularies
|
|
On April 4, CMS released its Medicare Program; Changes to the Medicare Advantage and the Medicare Prescription Drug Benefit Program for Contract Year 2024–Remaining Provisions and Contract Year 2025 Policy and Technical Changes to the Medicare Advantage Program, Medicare Prescription Drug Benefit Program, Medicare Cost Plan Program, and Programs of All-Inclusive Care for the Elderly (PACE) (CMS-4201-F3 and CMS-4205-F.) The final rule contains policies for Medicare Advantage (MA) and Medicare Part D plans in contract year (CY) 2025.
The policies finalized in this new rule include:
- New MA and Part D plan agent and broker compensation policies to guard against anti-competitive and anti-consumer steering,
- Limits to distribution of beneficiary data by Third-Party Marketing Organizations (TPMOs),
- Improvements in MA plan enrollee access to behavioral health care providers,
- Requirement of MA plan mid-year enrollee notifications for available supplemental benefits,
- New standards for MA special supplemental benefits for the chronically ill (SSBCI),
- Requirement that MA plans conduct plan-level annual health equity analysis of utilization management (UM) policies and procedures.
|
|
CMS Releases Final Rule for 2025 Qualified Health Plans, Aimed at Strengthening Network Adequacy, Patient Access and Protections and Improving Plan Selection and Enrollment |
|
On April 2, HHS and CMS issued the final Notice of Benefit and Payment Parameters for 2025 (CMS-9895-F).
The changes made by this rule include:
- Changes certain EHB prescription drug benefit requirements,
- Strengthening network adequacy by requiring State Marketplaces and State-Based Marketplace-Facilitated Programs (SBM-FPs) to establish quantitative time and distance qualified health plan (QHP) network adequacy standards,
- Allowing states to add routine adult dental services as Essential Health Benefits (EHB),
- Clarifying state-mandated benefits in state EHB-benchmark plans and defrayal.
|
|
For 2025, CMS Finalizes Changes Resulting in a 3.7% Increase in Plan Payments and Implements Inflation Reduction Act Provisions on Part D Benefit Redesign |
|
On April 1, CMS released its Announcement of Calendar Year (CY) 2025 Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies that would update program policies for Medicare Advantage and Medicare Part D beginning in 2025. CMS also issued its Final Calendar Year (CY) 2025 Part D Redesign Program Instructions which center on implementing provisions of the Inflation Reduction Act of 2022 (IRA) related to the Part D benefit for 2025.
Changes include:
- Changes to Effective Growth Rate and benchmark rate for MA payments,
- Changes related to implementing the IRA Part D benefit redesign for 2025,
- Continued phase-in of MA risk adjustment methodology,
- Continued risk adjustment model for Program of All-Inclusive Care for the Elderly (PACE) Organizations,
- Changes to the Part D risk adjustment model including IRA-related changes.
|
|
CMS Proposes FY 2025 Payment Update and Quality Changes for Inpatient Psychiatric Facilities (CMS-1806-P) |
|
On March 28, CMS issued the fiscal year (FY) 2025 Inpatient Psychiatric Facility Prospective Payment System (IPF PPS) and Quality Reporting (IPFQR) Updates proposed rule. In this rule, CMS proposes to:
- Increase IPF PPS payment rates by 2.7 percent,
- Revise the patient-level IPF PPS adjustment factors and increase electroconvulsive therapy (ECT) payment per treatment,
- Update the IPF wage index based on revised census data.
|
|
White House Releases Full Budget Request for Fiscal Year 2025, Proposing to Extend Medicare Trust Fund Solvency, Advance Health Equity, and Expand Access to Care While Lowering Costs |
|
On March 11, the White House released the President’s fiscal year (FY) 2025 budget, which builds upon the priorities included in the Infrastructure Investment and Jobs Act (Bipartisan Infrastructure Law), CHIPS and Science Act, and the IRA.
For HHS, the Administration is requesting $130.7 billion in discretionary funding and $1.7 trillion in mandatory funding. In a fact sheet regarding the FY 2025 budget request, HHS said: “The budget works to ensure all Americans have access to affordable healthcare; improve maternal and reproductive health outcomes; strengthen early care and education; address the needs of Indian Country; and advance scientific innovation.”
|
|
MACPAC and MedPAC updates |
|
Each March, the Medicaid and CHIP (Children’s Health Insurance Program) Payment and Access Commission (MACPAC) is required to report to Congress on the Medicaid program. In this report, MACPAC discusses engaging beneficiaries through Medical Care Advisory Committees to inform Medicaid policymaking, denials and appeals in Medicaid managed care, and its annual analysis of Medicaid disproportionate share hospital allotments to states. The report was released on March 15, 2024.
|
|
MedPAC Releases March 2024 Report to Congress |
|
Each March, the Medicare Payment Advisory Commission (MedPAC) is required to report to Congress on the Medicare fee-for-service (FFS) payment systems, the Medicare Advantage (MA) program, and the Medicare prescription drug program (Medicare Part D). In this report, MedPAC provides payment update recommendations for Medicare FFS payment systems, status updates on ambulatory surgical centers (ASCs), the MA program, and the Part D program; and mandated reports on dual-eligible special needs plans and rural emergency hospitals. The report also includes a chapter on estimating MA coding intensity and favorable selection. The report was released on March 15, 2024. |
|
MACPAC Holds March 2024 Meeting |
|
MedPAC Holds March 2024 Meeting |
|
On March 7 and 8, MedPAC held a virtual public meeting, which included the following sessions: Assessing data sources for measuring health care utilization by Medicare Advantage enrollees: encounter data and other sources; preliminary analysis of Medicare Advantage quality; rural hospital and clinical payment policy: a workplan for 2024-2025; and update on trends and issues in Medicare inpatient psychiatric services. |
|
What’s Next in Healthcare:
The Defining Trends to Follow
|
|
With election-year issues coming into focus, health policy is dominating much of the conversation in Washington. Pandemic-era telehealth flexibilities are set to expire at the end of the year, an end-of-year funding package looms in the near future, and the Biden Administration is advancing efforts to negotiate Medicare drug prices. Who will emerge as victors among the competing stakeholders in today’s healthcare debates?
On Wednesday, April 24, from Noon to 1 PM ET, Jonah Comstock, editor-in-chief of pharmaphorum; Ben Leonard, healthcare reporter at POLITICO; and John Wilkerson, Washington correspondent at STAT News, will join the Northern Virginia Health Policy Forum. Our panelists will share their insights on what is ahead in healthcare for Congress, providers, patients, and the industry.
|
|
Highlights from NVHPF's March Event:
Artificial Intelligence: Insights and Innovations in Tomorrow’s Healthcare
|
|
On March 20, the Northern Virginia Health Policy Forum welcomed Roberta Schwartz, PhD, MHS, Executive Vice President and Chief Innovation Officer at Houston Methodist Hospital, for a detailed discussion of AI in healthcare.
The Houston Methodist system, which includes a physician practice and academic medical center, serves seven million people in urban, rural, and suburban communities around Houston, Texas. Dr. Schwartz leads the Center for Innovation’s Digital Innovation Obsessed People team, which consists of health and technology professionals. With her front-line view, she shared insights on the implementation of AI at Houston Methodist and the broader healthcare system. Carl Mallory, Vice President of Healthcare Services at Applied Policy, led the conversation.
Watch highlights above, watch the event in its entirety here, or download a summary here.
|
|
Applied Policy was pleased to attend the Medtrade conference March 26-28 in Dallas, Texas, and to connect with friends in the industry. The largest home medical equipment (HME)/durable medical equipment (DME) trade show and conference in the U.S., Medtrade brings together HME/DME manufacturers and providers to create a forum for product sourcing, educational sessions, and networking across the industry. Attendees could choose several educational tracks, including audits and compliance; business operations; complex rehab technology; legislation, regulation, and legal; Medicare updates; payer relations; product development; and sales and marketing. |
|
HME providers have collectively struggled with supply chain and reimbursement challenges since the Covid-19 pandemic. Providers have also faced a host of supplier enrollment issues, such as revocation and corrective action plans, with the separation of the National Supplier Clearinghouse contract into two contracts, Palmetto GBA and Novitas Solutions, in November 2022. Medtrade offered a space for providers and manufacturers to connect about how to overcome these pressures, offer new solutions, and advocate for patients. |
|
A Warm Welcome to Our New Intern |
|
We are happy to welcome Annie Tuttle as the newest addition to our intern team. Annie, who graduated from the College of William and Mary last year, is currently pursuing her master’s in public policy at The George Washington University.
Annie believes that her work at Applied Policy will position her to pursue her goal of continuing to work in the policy space in the future.
|
|
She observed that she "wasn’t expecting the level of support and education that Applied Policy provides interns.”
In the rare moments Annie isn't immersed in her work or studies, you might find her in the pool or hitting the pavement. Having been a competitive swimmer for years, she found that she also enjoys running. In fact, she recently crossed the finish line of her first half marathon.
|
|
On the Docket/Under Review |
|
Applied Policy is following these rules under review at the Office of Management and Budget:
- Occupational Exposure to COVID-19 in Healthcare Settings
- Healthcare System Resiliency and Modernization (CMS-3426)
- Alternative Payment Model Updates; Increasing Organ Transplant Access (IOTA) Model (CMS-5535)
- Medicaid and Children's Health Insurance Program (CHIP) Managed Care Access, Finance, and Quality (CMS-2439)
- Nondiscrimination in Health Programs and Activities
- Health Data, Technology, and Interoperability: Patient Engagement, Information Sharing, and Public Health Interoperability
- Ensuring Access to Medicaid Services (CMS-2442)
- Minimum Staffing Standards for Long-Term Care Facilities and Medicaid Institutional Payment Transparency Reporting (CMS-3442)
- Medical Devices; Laboratory Developed Tests Final Rule
- Rulemaking on Discrimination on the Basis of Disability in Health and Human Services Programs or Activities
- Misclassification of Drugs, Program Administration and Program Integrity Updates Under the Medicaid Drug Rebate Program (CMS-2434)
See all rules under OMB review here.
|
|
April 9-12
April 14-16
April 15-18
April 17-19
May 14-16
May 21
|
|
JAMA
Precision Medicine Online
Reuters
|
|
Insight Joke of the Month for April |
|
What kind of doctor fixes websites? |
|
Tuning into Policy:
The Tradeoffs Podcast
|
|
Produced to enlighten healthcare leaders, policymakers, and consumers, the Tradeoffs podcast combines engaging storytelling with rigorous data analysis to explain healthcare's complexities and costs.
Recent episodes have considered bipartisan efforts to better serve individuals eligible for both Medicare and Medicaid, the anticipated influence of America's judiciary on healthcare in 2024, and the impact of the No Surprises Act on patients and providers.
|
|
*False. The Pickle hospital designation is specific to the Medicare DSH program. It takes its name from the late Texas congressman James Jarrell Pickle. Learn more in our Medicare DSH deep dive above.
|
|
|
|
|
Applied Policy, L.L.C., is a health policy and reimbursement consulting firm strategically located minutes from Washington, D.C.
|
|
|
|
|
|
|