|
Background
Sulfonylureas are insulin secretagogues used in the management of Type 2 diabetes mellitus. The first generation (acetohexamide, chlorpropamide, tolazamide, and tolbutamide) are no longer widely used and have largely been replaced by the second generation sulfonylureas (glimepiride, glipizide, and glyburide). Second generation sulfonylureas are more potent and can be administered in lower doses once daily (Costello et al, 2023). Some sulfonylureas are formulated with metformin or the thiazolidinediones.
Mechanism of Toxicity
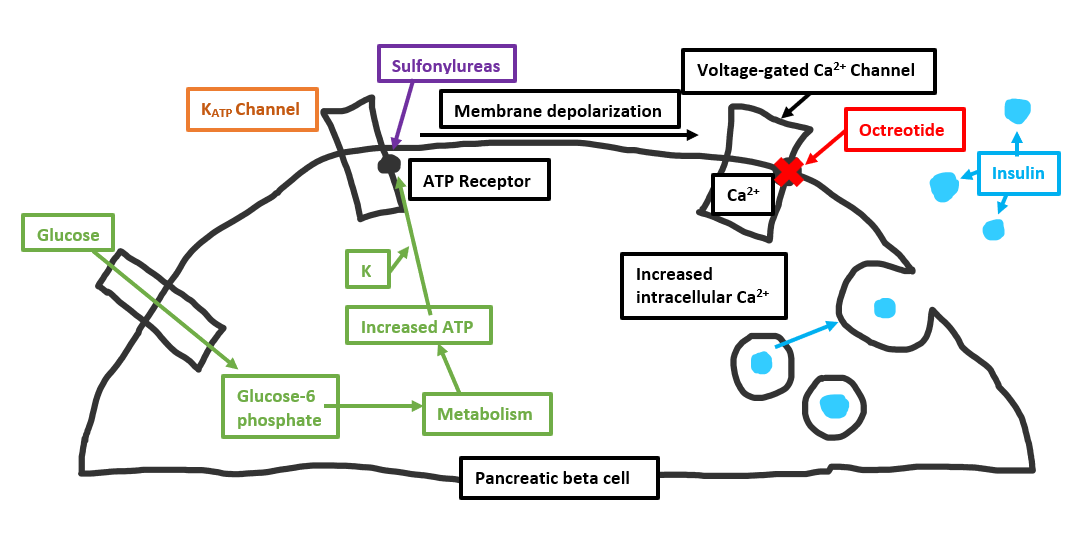
Sulfonylureas bind to the pancreatic beta cell and cause a closure of the K+ channels. Inhibition of potassium efflux mimics the effect of naturally elevated intracellular ATP and causes membrane depolarization. The subsequent rise in intracellular potential opens the voltage gated calcium channels, which increases the intracellular calcium concentration. The increase in calcium results in the release of insulin and subsequently hypoglycemia (Bosse GM, 2019).
Clinical Presentation
All sulfonylureas in overdose cause hypoglycemia and associated neuroglycopenia. The risk for hypoglycemia is greater in drug naïve patients, especially young children. The onset of hypoglycemia varies depending on multiple factors (e.g. timing of the last meal or available glycogen stores) and can be significantly delayed (Bosse GM, 2019).
|