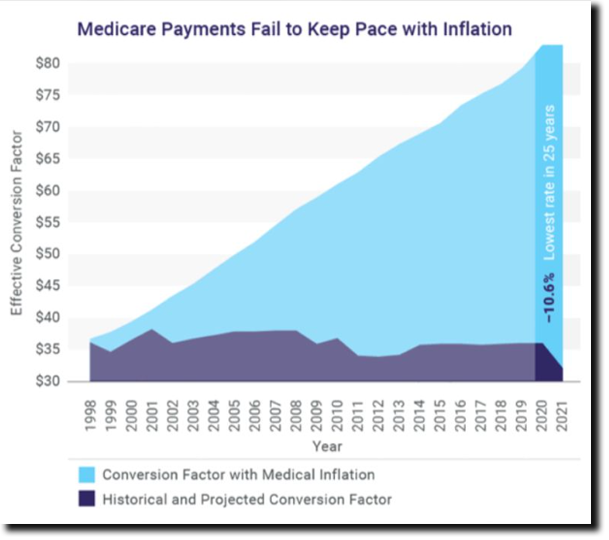
Compounded by an escalating 9% inflation, this equals a 20% cut!
This is worse than we expected. Your survival is at stake - respond now!
Join ASIPP's effort to reverse these alarming trends by clicking here.
|
|
|
To see sample rates compared to 2022, click here. In addition to the 4.4% cuts, some codes have faced higher reductions with very few codes facing increases. The same applies to 10.4% cuts.
In reference to ASCs, as of now, they are not proposing any cuts; however, a 6% cut will remain in effect unless the 2% sequester cut from ACA and 4% statutory PAYGO from the American Rescue Plan Act are eliminated.
The fee schedule remains stable except for a few small increases. Some of the procedures that received major increases include sacroiliac joint arthrodesis and moderate increases for peripheral nerve stimulators.
|
|
June’s modest volume and expense improvements were not enough to pull the hospital industry’s median operating margin into the green, marking six straight months of negative operations across the country, according to a new industry report.
Hospitals and health systems saw a median 30.8% improvement in their operating margins from May to June, leading to a median year-to-date operating margin index of -0.09%, according to Kaufman Hall’s numbers through June.
Despite the upward trend, the firm wrote that the industry still lags well behind the midpoint of 2021, is “nowhere near pre-pandemic levels” and “will likely end up with historically low margins for the remainder of the year.”
|
|
Register today for the CALSIPP Annual Meeting and join us for an Evening Cruise on the Bay!
Saturday, October 15 | 7:30 pm
|
|
Enjoy an entertaining three-hour yacht cruise around Newport Bay on a two-level contemporary yacht. Take in the beautiful sights from the outdoor viewing areas on the large bow, aft deck, or by strolling the walk-around decks.
Limited tickets are available, so do not wait! Tickets are $100 per registered meeting attendee or guest and must be selected on the registration form.
Register for the meeting and select the Cruise Add On.
|
|
Recommends wearing a mask for 10 days and testing on or after day 5 instead
Instead of quarantining if you're exposed to COVID-19, wear a high-quality mask for 10 days and get tested on or after day 5, irrespective of vaccination status, the CDC suggested in revised COVID guidelines issued Thursday.
"In light of high population levels of anti–SARS-CoV-2 seroprevalence, and to limit social and economic impacts, quarantine of exposed persons is no longer recommended, regardless of vaccination status," Greta Massetti, PhD, of the CDC COVID-19 Emergency Response Team, and colleagues wrote in Morbidity and Mortality Weekly Report.
In addition, "CDC now recommends case investigation and contact tracing only in healthcare settings and certain high-risk congregate settings," the authors wrote. The updated guidelines no longer mention the "test to stay" strategy previously recommended for school students who had a potential exposure.
|
|
No additional cases identified, but wastewater testing continues to detect the virus
No additional U.S. cases of poliomyelitis have been identified, according to a new CDC report detailing the nation's first case in nearly a decade, but wastewater specimens in multiple New York counties indicate community transmission and ongoing risk for paralysis in the unvaccinated.
Following stool sample testing, poliovirus was confirmed in June in an unvaccinated young adult from Rockland County, New York, representing just the second case of local transmission in the U.S. since 1979.
The patient had initially experienced fever, neck stiffness, gastrointestinal symptoms, and weakness in the limbs, and was hospitalized for possible acute flaccid myelitis (AFM), reported Ruth Link-Gelles, PhD, of the CDC's Domestic Poliovirus Emergency Response Team, and colleagues in the Morbidity and Mortality Weekly Report.
|
|
NEXT EXAM DATES:
Part I
August 27, September 17,
October 22, November 19 & December 17
Part II
September 23
|
|
National data outlines factors behind racial and sex-based disparities
Racial and sex-based disparities in prevalence of gout may be explained by differences in diet, kidney health, and other key risk factors, a cross-sectional study found.
After age-standardization, the prevalence of gout among Black women was 3.5% compared with 2.0% among white women (age-adjusted OR 1.81, 95% CI 1.29-2.53), according to findings in JAMA Network Open. Among Black men, the age-standardized prevalence of gout was 7.0%, whereas the prevalence was 5.4% among white men (age-adjusted OR 1.26, 95% CI 1.02-1.55).
However, all risk factors for gout were more common among Black adults than white adults, reported Natalie McCormick, PhD, of Massachusetts General Hospital in Boston, and colleagues.
|
|
Shifting the paradigm around prescribing opioids
From ancient precepts such as the Hippocratic Oath promising to abstain from doing harm to the modern bioethics principle of nonmaleficence, the calling of physicians involves striving to help alleviate suffering and avoid making it worse. But in our increasingly complex healthcare and data environment, avoiding inadvertent harm can be more difficult than one might expect.
I attended medical school in the late 2000s and completed my residency training in orthopedic surgery during the first half of the 2010s. It was a decade during which pain was emphasized as a "fifth vital sign," placing it in the hierarchy of crucial indicators of being alive, along with heart rate, blood pressure, temperature, and respiratory rate. Pain had historically been undertreated in a system that was not patient-centered, and patient advocates rightly lobbied for increased attention to this aspect of the patient experience.
Unfortunately, the medical community's response to this deficiency was pharmaceutically-based and lacking in nuance. Spurred on by the insidious actions of the manufacturers of opioid medications, these drugs assumed a far too prominent role in the treatment of pain. We were told repeatedly in medical school that one could not become addicted to a drug so long as it was administered to treat pain and that addiction was only a risk when opioids were consumed in the absence of pain. This turns out to be patently untrue.
|
|
Drugmakers are launching new medicines at record-high prices this year, a Reuters analysis has found, highlighting their pricing power even as Congress moves to cut the $500 billion-plus annual bill for prescription drugs in the United States. At the same time, some pharmaceutical manufacturers are disclosing less information about the pricing of those treatments, which have come under greater scrutiny in recent years, Reuters found.
"In the U.S. we allow drug manufacturers to freely set prices for all brand-name drugs," Dr. Aaron Kesselheim, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital, told Reuters.
The median annual price of 13 novel drugs approved for chronic conditions by the U.S. Food and Drug Administration so far this year is $257,000, Reuters found.
|
|
|
|
Please plan to join us at the
2023 ASIPP Annual Meeting
March 16-18 National Harbor, Maryland
Register Early
More details will be posted on our website at asipp.org.
Registration begins November 2022.
|
|
For meeting or exhibitor/sponsor information:
|
|
- ASIPP Members Only Site Information - |
|
-
To log in for the first time you will need to click “forgot password” at the bottom of the login window.
- Check your email and then log in as directed.
-
If you have problems logging into your account, click here.
|
|
Pain Medicine Case Reports (PMCR) and Editor-in-Chief Alaa Abd-Elsayed, MD, PhD would like to invite you to submit case reports and case series to the PMCR journal. Your article will be published free of charge.
Open access journals are freely available online for immediate worldwide open access to the full text of published articles. There is no subscription fee for open access journals. Open access journals are no different from traditional subscription-based journals: they undergo the same peer-review and quality control as any other scholarly journal.
Interested in becoming a member of the PMCR Editorial Board?
Editorial board members are asked to review 2-6 manuscripts per year. Please submit your most up-to-date CV to sgold@asipp.org for consideration.
For more information or to submit your articles, click here.
|
|
| CASE REPORT |
Jyotsna Punj, MD, Longjam Darendrajit Singh, MD, Heena Garg, MD, Dhruv Jain, MD, Jay Prakash Thakur, MD, and Gaurav Gomez, MD
Abstract
BACKGROUND: We describe a new method of ultrasound-guided lumbar transforaminal injection with an electrical stimulation needle (NsUTFI) in 2 patients with disc herniation at the L5-S1 and L4-L5 levels, respectively. The patient provided HIPAA compliant consent for the inclusion of their clinical information in this report.
CASE REPORT: NsUTFI was performed by eliciting sensory and/or motor stimulation of nerve roots by an electrical stimulation needle, which was inserted in an out-of-plane (OOP) trajectory just beyond the intertransverse ligament between the appropriate 2 transverse processes via a paramedian sagittal oblique (PSO) approach with a curved probe. Fluoroscopic confirmation was not done. Both patients reported 50% pain reduction at 2 weeks’ follow-up.
CONCLUSION: We conclude that a new technique for lumbar radicular pain with NsUTFI with a PSO OOP needle trajectory at the intertransverse ligament may be safe and effective and should be further explored.
KEY WORDS: Electrical stimulation, paramedian sagittal oblique, transforaminal injection, ultrasound
|
|
| RANDOMIZED TRIAL |
Matthias Hubert Morgalla, MD, PhD, and Lydia Domay, MD
Abstract
BACKGROUND: In the presence of neuropathic pain, other sensory qualities, such as touch or pressure, which are a sign of nerve damage, are almost always affected. However, it is unclear to which extent spinal cord stimulation (SCS) influences these simultaneously damaged sensory pathways or possibly contributes to their regeneration.
OBJECTIVES: The aim of this study was to investigate the effects and possible differences of tonic and BurstDR (Abbott, Austin, TX) SCS on somatosensory profiles of patients with chronic neuropathic pain, using quantitative sensory testing (QST).
STUDY DESIGN: A randomized, single-blinded, single-center study.
SETTING: University medical center.
METHODS: After a washout phase of 4 hours and having done the basic QST measurement, either tonic or BurstDR stimulation was performed for 30 minutes in a randomized fashion. Then, the second measurement was taken. The third measurement followed after using the remaining stimulation mode for 30 minutes. Mean values of all QST parameters were calculated and compared. We also computed Z-values using standard data.
RESULTS: We examined 14 patients (9 women, 5 men, mean age 58.4 years) with previously implanted SCS systems for chronic neuropathic pain, using QST (7 tests, 13 parameters).
The QST raw data showed a statistically significant improved vibration sensation (A-Beta) (P = 0.019) and lower mechanical pain threshold (A-Delta) (P = 0,031) when testing BurstDR in comparison to tonic SCS. We found a significant improvement in the vibration sensation and also A-Beta fiber function during BurstDR when we used the Z-value analysis (P = 0.023). With regard to Z-values, BurstDR seemed to be superior regarding the normalization tendency of the A-Delta fiber function in the mechanical pain threshold (P = 0.082), and tonic SCS seemed superior regarding heat detection threshold (C) and cold pain threshold (C and A-Delta) (P = 0.093).
LIMITATIONS: The study is limited by its small number of cases.
CONCLUSIONS: In this study, it could be shown that, in some QST parameters and tested fiber functions, normalization tendencies were recognizable by using BurstDR or tonic SCS. However, BurstDR SCS seemed to be superior to tonic stimulation in this regard.
KEY WORDS: Quantitative sensory testing, spinal cord stimulation, neuropathic pain, BurstDR stimulation, tonic stimulation, Z-transformation
|
|
| PROSPECTIVE STUDY |
Amol Soin, MD, David Barrall, MD, Joe Chen, MD, Anu Patel, MHCDS, Ann Pollack, MHCDS, and Amos Wangombe, MHCDS.
Abstract
BACKGROUND: In the United States, the prevalence of opioid use disorders has increased in recent years along with an attendant rise in the incidence of chronic pain disorders and prescription opioid use. Patient navigation services have been used to improve health outcomes in cancer and other chronic disease states, but it is unclear whether the implementation of patient navigation services can facilitate improved outcomes among patients receiving chronic opioid therapy.
OBJECTIVES: The objective of this study was to compare the outcomes of patients receiving chronic opioid therapy plus patient navigation services and those receiving chronic opioid therapy as a part of usual care.
STUDY DESIGN: This was a prospective, observational study. Consecutive patients receiving chronic opioid therapy were enrolled, with alternating assignments to patient navigation (n = 30) or usual care (n = 30). Participants in the patient navigation group received support from a non-physician, non-advanced practice provider staff member who initiated frequent contact via telephone, telemedicine, or in-clinic visits to discuss the patient’s health goals. The minimum follow-up period was 90 days. Outcomes qualitatively compared across groups included final pain score, final morphine milligram equivalent (MME) per day, and discharge rates. Risk factors for discharge within the navigation group were assessed. Patient feedback was also solicited.
SETTING: This study was conducted at a single independent pain clinic in the United States.
RESULTS: Demographic features were similar between the navigator group and the control group. The control group had a higher average initial pain score (7.0/10) than the intervention group (5.9/10) and were receiving a higher initial dose of opioids (23.1 vs 19.0 MME/d). After an average follow-up of 108.7 days, patients in the navigator group had a 16% decrease in final opioid dose compared with a 23% increase in the control group. Furthermore, patients in the control group were discharged from the practice at a higher rate (23.3% vs 6.6%), suggesting increased opioid misuse in the control group compared with the navigator group. In the navigator group, higher levels of anxiety and depression were the primary predictors of discharge.
LIMITATIONS: This was a single-center study with a small sample size. The generalizability of these results to other clinic settings is unknown.
CONCLUSIONS: Patient navigation decreased opioid use and practice discharge compared with usual care in an independent pain clinic, suggesting a role for patient navigation in reducing opioid misuse and potentially reducing adverse events.
KEY WORDS: Opioid prescribing, patient navigation, Opioid Risk Tool, opioid nonadherence, anxiety, depression
|
|
Since this malpractice insurance program officially launched in November 2018, ASIPP has signed up hundreds of providers with an average savings of 30%. This is professional liability insurance tailored to our specialty and will stand up for us and defend our practices.
Norcal Mutual is A-Rated by AM best and is licensed in all 50 states. To read a few important points to keep in mind about the program, including discounts, administrative defense, cyber coverage, aggressive claims handling, and complimentary award-winning risk management CME activities, click here.
|
|
ASIPP® has formed a partnership with Henry Schein and PedsPal, a national GPO that has a successful history of negotiating better prices on medical supplies and creating value-added services for independent physicians. Working with MedAssets, PedsPal provides excellent pricing on products like contrast media that alleviate some of the financial pressures you experience today.
|
|
ASIPP® is now offering our members the benefit of a unique revenue cycle management/ billing service.
We have received a tremendous amount of interest in the ASIPP® billing and coding program.
Click here to learn more about the negotiated rate for practices and more!
|
|
|
up-to-date news related to you, your practice, and your patients!
|
|
|
|
|
|
|