Appropriate lymphadenectomy during esophagectomy allows for accurate staging and may also impact long-term survival. The presence of lymph node (LN) metastasis remains a key indicator in the management and prognosis of esophageal cancer.
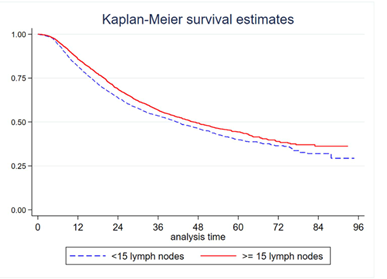
Given the importance of surgical lymphadenectomy, the purpose of this study was to determine the rate and predictors of appropriate lymphadenectomy among patients receiving MIE. Patients receiving MIE in the National Cancer Database from 2010 to 2016 were identified. There were 6,539 patients who underwent MIE from 2010 to 2016 in the NCDB and met inclusion criteria. The mean number of LNs resected was 16.2 (median 15, IQR 9–22). Overall, 3,527 (53.9%) received adequate lymphadenectomy and the remaining 3,012 (46.1%) did not. At multivariable regression, factors associated with adequate lymphadenectomy were institutional volume of MIE, performing MIE at an academic center and presence of clinical nodal disease. Multivariable Cox proportional hazard analysis demonstrated a survival benefit with adequate lymphadenectomy in the overall cohort, among patients receiving neoadjuvant therapy, and in patients who did not receive neoadjuvant treatment.