Physician Advisors: To Practice, Or Not To Practice |
Basics of Medicare-Severity Diagnosis Related Group (MS-DRG) |
The Inpatient Only List Reinstated |
Yes, You Can Admit Psychiatric Cases as Inpatients
|
Can a Patient with Sepsis Be Discharged from the ED? |
|
|
|
|
Ronald Hirsch, MD, FACP, CHCQM-PHYADV, CHRI
Member, ACPA Advisory Board
Editor, ACPA Update
|
|
I hate to have to start this month’s newsletter with a scolding, but it is necessary. What the heck members?? Only 17 ACPA members have responded to the February Observation Committee cases. Yeah, I know, we are in the midst of a pandemic, provider burnout is at an all time high, and the last thing you want to do is answer some silly quiz. Don’t be that person. It reminds me of a time a patient was hospitalized with a GI bleed who had a recent cardiac stent. The hospitalist was discharging the patient but not resuming any anti-platelet agents. I asked him if he had read the recent New England Journal of Medicine about the safety of resumption of these medications if the bleeding was controlled and his response was “I am too busy to read journals.” No wonder it can often take years for disproven therapies to stop being used by doctors. Keep learning new things, keep unlearning obsolete things, keep challenging yourself. Now go and do the cases now: https://www.surveymonkey.com/r/GKGYDFY
This month’s issue is another great one. Two Midnight Rule, Sepsis, DRGs, Psychiatric Admissions, Balancing Administrative and Clinical Time are all timely topics. Let me remind you that every article was written by an ACPA member who received no compensation for their time and effort. Their reward, and my reward for editing this newsletter, is knowing that we are furthering the knowledge base of our colleagues and working to increase the respect and recognition of the role of the physician advisor.
So please take the time to read every article and if you have a spare moment or two, go to the ACPA webpage www.acpadvisors.org, sign in, look up the author in the member directory, and drop them a quick thank you note. If you are a member of RAC Relief user group, post a note there about the article. I would also welcome any “letters to the editor” addressing any of the articles and will publish them in a future issue. And of course you are always welcome to submit an article for the ACPA newsletter. Email me at signaturedoc@gmail.com for the submission guidelines.
|
|
|
|
Physician Advisors: To Practice, Or Not To Practice |
Clarissa Barnes, MD, CHCQM-PHYADV, FACP
Vice President Member Engagement, ACPA
|
|
The struggle between clinical practice and physician advisor duties is as old as the physician advisor role itself. Dr. Ronald Hirsch recently wrote an article exploring some of the pros and cons to continuing a clinical practice on RACmonitor.com. It’s an excellent look at the range of considerations. In addition to personal considerations, there are employment considerations that may make continuing a mix more palatable from a work-balance perspective as well as improve your ability to attract new talent and protect yourself from staffing issues.
Where you are in your career often makes a big difference in what you are personally willing to do and what others you may want to hire are willing to do. As many of us know (and the recent American College of Physician Advisor survey confirms), many physician advisors are new to this work. Often, they have little experience before they start. It can be quite difficult for someone to make the jump to full-time physician advisor work when they’ve never done physician advisor work before. It is hard to “give up” clinical work (even if you want to or think you are ready) when you are still not sure what you’re getting in return. I have seen physician advisor job postings attract little interest at one position at 1.0 FTE but get multiple applicants when offered as 5 positions of 0.2 FTE.
Splitting up FTE works well in recruiting new candidates to the physician advisor field because it allows them to try it out so they can be comfortable that this is work they enjoy. If it does not work out and they leave their physician advisor role, it also benefits the hospital or health system because it is a lot easier to flex up to cover the 1 day a week they have left open than have to start all over again finding a full-time person.
Ultimately some of the strongest arguments against continued clinical practice stem from the inherent nature of having multiple roles. Namely, it can be hard to compartmentalize and what should be two roles you alternate between often becomes two roles you fill simultaneously. The solution can be to stop doing one role and take up the other full-time. However, there are other options that allow you to keep your jobs separate and preserve your sanity. Specifically, the model stated above where 5 people split 1.0 FTE of physician advisor work so that everyone works one day a week works well when you have physician advisors who want to keep their clinical roles. If their clinical roles are shift-work oriented such as hospitalist or emergency physicians, they can keep their roles distinct and these preserved boundaries help promote work-life balance.
The added benefit of physician advisors who still practice clinically is that they take anything they learn back to their practice group. For example, recently two of the newer physician advisors at my hospital found themselves working clinical as ER physician and admitting hospitalist. They had an entire discussion with each other about antibiotic selection for pneumonia and how that meant they should document that they were concerned about gram negatives as a cause instead of a “simple pneumonia” based on their recent educational exposure as part of their physician advisor training. Obviously, physician advisors will educate other physicians as part of their administrative time, but real-time education and discussion because your physician advisors are also seeing patients can be priceless.
In the interest of full disclosure, as someone who is mid-career, my FTE between administrative and clinical duties seems to be constantly in flux and the decision on how much time to devote to each is one I seem to struggle with constantly. I anticipate a time where it will be too difficult to maintain the amount of clinical time I have currently, but there are ways to make it work so that you don’t get burned out and there are benefits to keeping a presence in both worlds.
Dr. Barnes is a System Physician Advisor for Avera Health in Sioux Falls, SD.
|
|
|
|
Basics of Medicare-Severity Diagnosis Related Group (MS-DRG) |
Ahmed Abuabdou, MBBS, MBA
Vice President – Operations, ACPA
|
|
Medicare Severity Diagnosis Related Group (MS-DRG) understanding is an essential area of knowledge for us as physician advisors. While it is the most common payment methodology for inpatient level of care in the current landscape, some physicians, early career physician advisors and hospital executives might not have a good understanding of what MS-DRG is and what are the several variables which could impact the correct DRG assignment.
Here is some basic information about MS-DRG
Diagnosis Related Group is defined as patient classification system that provides a methodology for relating the type of patients a hospital treats (i.e., its case mix) to the costs incurred by the hospital.1
The current version of MS-DRG is v39 (accessed here: https://www.cms.gov/icd10m/version39-fullcode-cms/fullcode_cms/P0001.html) and it contains 765 DRGs. These DRGs are structured within the framework of 25 Major Diagnostic Categories (MDCs) and an extra category called pre-MDC. Most MDCs contain surgical and medical MS-DRGs, depending on what the principal diagnosis is and whether there is an operative procedure. Diagnoses are offered in the current classification system, currently International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Procedures are recorded in the inpatient Procedure Coding System known as ICD-10-PCS.
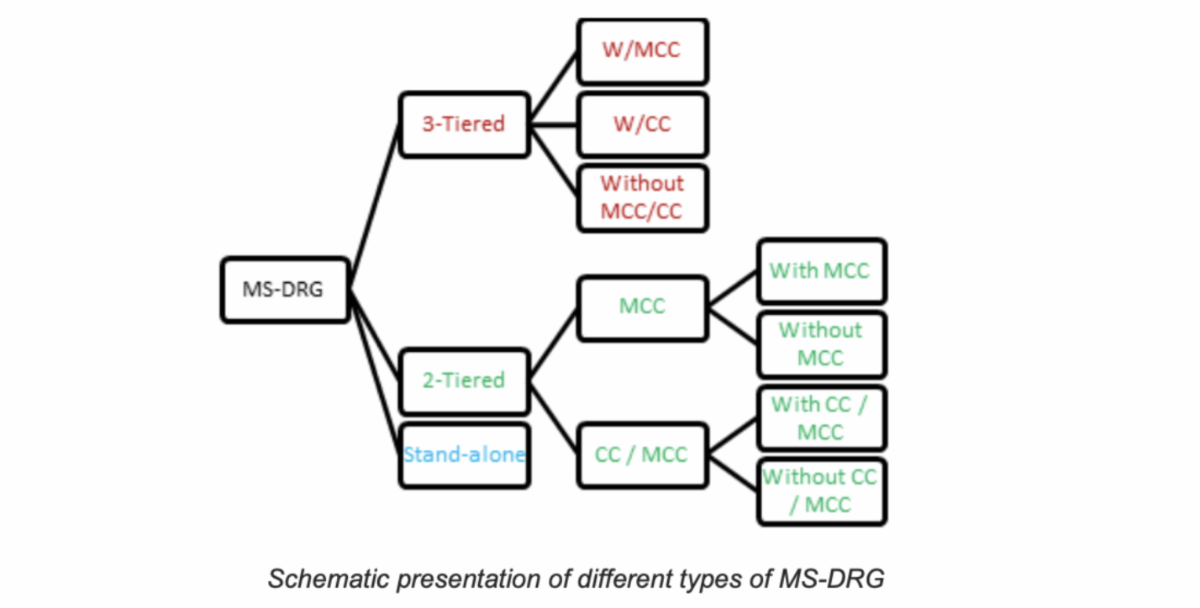
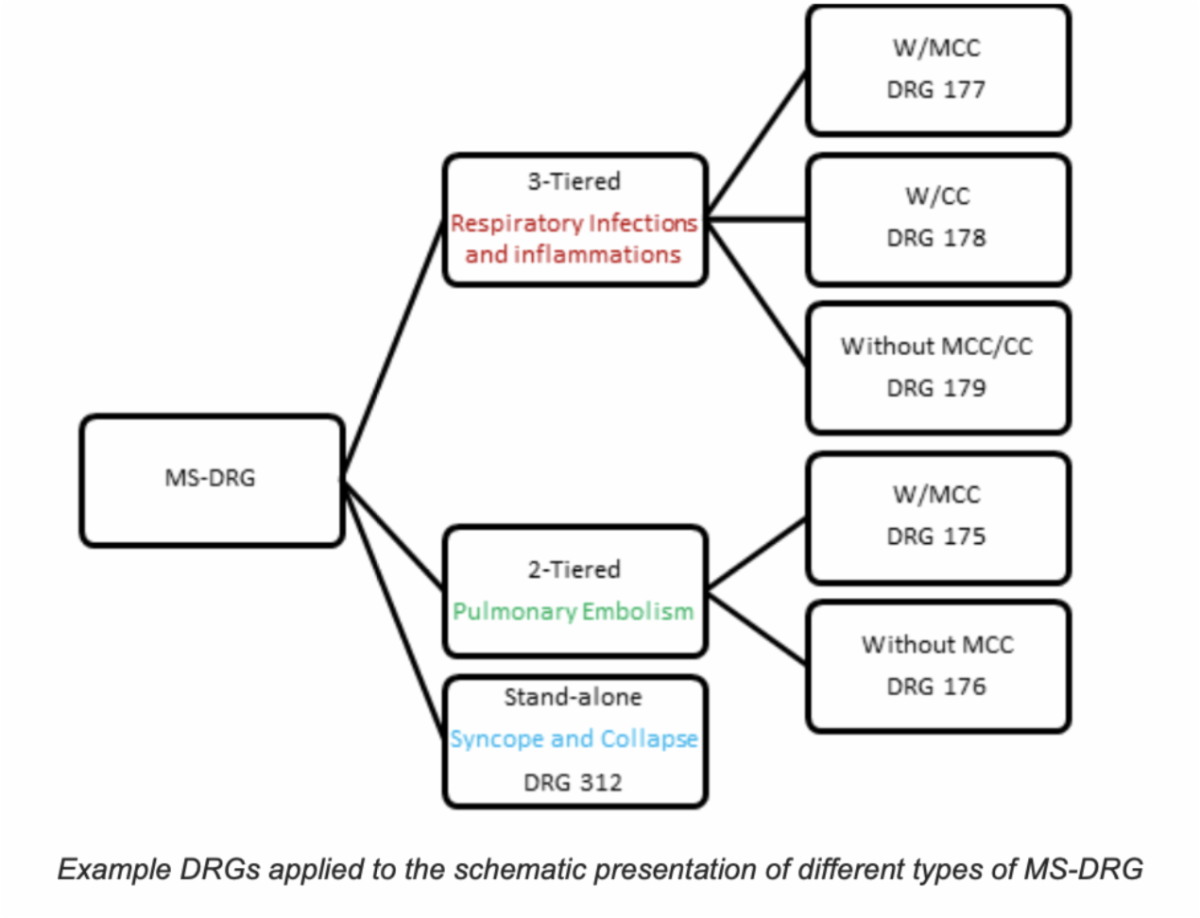
MS-DRG can be 3-tiered DRGs, 2-tiered DRGs, or standalone DRGs as shown in the schematic representation below:
|
|
The anatomical components of MS-DRG include:
1) Principal Diagnosis
Uniform Hospital Discharge Data Set (UHDDS) defines Principal Diagnosis (PDx) as the condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care. This may not be identical to the admitting diagnosis (e.g., admitted for abdominal pain but, after study, PDx is determined to be acute cholecystitis).
For the most part, the principal diagnosis drives the DRG assignment. On certain occasions where a surgical procedure is performed, or pregnancy status is reported, the principal diagnosis might not be the sole driver for the DRG assignment. Secondary diagnoses impact the DRG assignment as well by adding a CC and/or MCC when clinically valid, supported, and consistently documented.
2) Secondary Diagnoses
UHDDS defines secondary diagnoses as all conditions that coexist at the time of admission, that develop subsequently, or that affect treatment received and / or length of stay.
3) Comorbid Conditions or Complications
Some secondary diagnoses are designated as risk-adjusting comorbid conditions or complications (CCs). Others considered even more serious are referred to as major comorbid conditions or complications (MCCs). CCs and MCCs indicate a higher severity of illness, risk of mortality, and intensity of resource utilization. These CCs and MCCs define many of the tiered MS-DRG sets. It only takes one CC or MCC to establish the tier. Although it is optimal to capture all the CCs/MCCs present, having more than one in a given tier does not have any greater impact.
Examples of CCs include chronic respiratory failure (hypoxemic, hypercapnic, or combined), chronic congestive heart failure (systolic, diastolic, or combined), acute kidney injury, hyponatremia, and moderate protein-calorie malnutrition. Examples of MCCs include acute or acute on chronic respiratory failure (hypoxemic, hypercapnic, or combined), acute or acute on chronic congestive heart failure (systolic, diastolic, or combined), pneumonia, and severe protein-calorie malnutrition.
4) Relative Weight (RW)
RW is a measure which reflects the relative resource consumption (cost) associated with treatment of that condition as compared to the resource consumption of the average Medicare patient (by convention, defined as 1.0000). Each DRG is assigned a specific RW. The Medicare Payment Advisory Committee (MedPAC) reviews hospital claims data annually as part of IPPS annual updates resulting in changes to RW each year. In MS-DRG sets, the relative weight increases with the tier; e.g., RW of DRG with MCC > RW of DRG with CC > RW of DRG without CC or MCC.
5) Case Mix Index (CMI)
CMI is a numeric measure which represents the average DRG RW for that hospital. It is calculated by summing the DRG weights for all Medicare discharges and dividing by the number of discharges. It is used to find and adjust the average care cost per patient at a hospital based on the patient population demographics. For example, if a hospital’s average cost per patient is $2,000 and its annual CMI is 0.90, then the adjusted cost per patient would be $2,222.22. In general, increased capture of MCCs equates to higher CMI. Higher surgical DRGs results in higher CMI as well. To put it in simple words, higher CMI means you are treating sicker, more complex, and more resource-intensive patients.
6) Hospital Base Rate
Hospital Base Payment Rate (Blended Rate) is a monetary number assigned to an individual hospital that allows for adjustment according to individual characteristics of that hospital. It is recalculated annually to reflect differences in operating expenses as well as capital expenses. Factors that impact the hospital blended rate include proportion of indigent population, capital costs, wage index, urban vs rural designation, teaching vs non-teaching designation, and cost of living adjustments. The Hospital Base Rate multiplied by the RW of the MS-DRG determines the payment for a given patient encounter.
7) Length of Stay (LOS)
Arithmetic Mean Length of Stay (ALOS) reflects the average LOS for CMS patients who fall into a given MS-DRG. Geometric Mean Length of Stay (GMLOS) reflects the average LOS for CMS patients who fall into a given MS-DRG with patients with abnormally short or long LOS (called outliers) being removed from the calculation. In tiered DRG sets, the higher the tier, the longer the allotted LOS.
The basic equation which explains the MS-DRG payment is shown below. While we (physicians and physician advisor community) have no direct control over what the updated hospital base rate would be every year, we have control in documenting all clinically relevant and pertinent diagnoses which can risk adjust the MS-DRG (if designated as MCC or CC) leading to a higher RW which will ultimately lead to higher reimbursement.
|
|
In certain cases an add-on payment is included such as Disproportionate Share Hospital (DSH) adjustment for indigent population, Indirect Medical Education (IME) adjustment, and outlier payment for considerable amount of facility resources (such as drugs and technology).
The MS-DRG and its variables such as Relative Weight (RW), Geometric Mean Length of Stay (GMLOS), designating a secondary diagnosis as Major Comorbidity / Complication (MCC) or Comorbidity / Complication (CC) among several others, are updated yearly as part of the Inpatient Prospective Payment System (IPPS) final rule (effective for discharges occurring on October 1st of each calendar year).
Physician advisors are in a unique position to assist hospitals or health systems improve their quality metrics and reimbursement. Although improving efficiency and delivery of medical care by being good stewards of resource utilization is of the utmost importance, implementing documentation improvement strategies to optimize the DRG, risk adjustment, and reimbursement can be extremely valuable as well..
References:
Dr. Abuabdou is a practicing Hospital Medicine faculty at the University of Arkansas for Medical Sciences, Little Rock, Arkansas. He serves as Associate Chief Medical Officer for UAMS Medical Center and leads its Physician Advisory Program.
|
|
|
|
The Inpatient Only List Reinstatedi
|
Jessica L. Gustafson, Esq.
ACPA Advisory Board Chair and Member
Abby Pendleton, Esq.
ACPA Advisory Board Member
|
|
I. Introduction
One year after deciding to phase out the inpatient only (IPO) list entirely, the Centers for Medicare & Medicaid Services (CMS) reversed course. Noting stakeholders’ concerns related to patient safety in rendering certain procedures on an outpatient basis, CMS concluded that the IPO list should remain in effect. Effective January 1, 2022, CMS returned the vast majority of services removed from the IPO list in 2021 (except for CPT codes 22630 (Lumbar spine fusion), 23472 (Reconstruct shoulder joint), 27702 (Reconstruct ankle joint) and their corresponding anesthesia codes) and halted the phase out of the IPO list.ii
II. Discussion
A. The History of the IPO List
The IPO list was established in the first Medicare Program Prospective Payment System for Hospital Outpatient Services final rule in 2000.iii The IPO list identifies services for which Medicare will only make payment if they are performed in the inpatient hospital setting due to the nature of the procedure, the underlying physical condition of the patient, or the need for at least 24 hours of postoperative hospital care for recovery or monitoring before the patient can be safely discharged.iv The procedures included on the IPO list include services that, in the view of CMS, “would not be safe, appropriate, or considered to fall within the boundaries of acceptable medical practice” if they were performed in the outpatient setting.v Although the inclusion of a service on the IPO list does not prohibit the service from being rendered in the outpatient setting, Medicare will not render payment for the service if it is performed in the outpatient setting.vi On the other hand, if a service is not included on the IPO list, the service is not precluded from being reimbursed in the inpatient hospital setting; rather, the procedure may be provided, and CMS may provide reimbursement for the procedure, in either the inpatient or outpatient settings.vii
In establishing the IPO list, CMS noted that, “In the future, as part of our annual update process, we will be working with professional societies and hospital associations, as well as with the expert outside advisory panel… to reevaluate procedures on the ‘inpatient only’ list and we will propose to move procedures to the outpatient setting when we determine it to be appropriate.”viii Historically, CMS has effectuated such removals from the IPO list gradually, based on evolution of acceptable medical practice. The criteria for evaluating whether to remove a procedure from the IPO list included the following:
- Most outpatient departments are equipped to provide the services to the Medicare population.
- The simplest procedure described by the code may be performed in most outpatient departments.
- The procedure is related to codes [CMS has] already moved off of the inpatient list…
- [T]he procedure is being performed in numerous hospitals on an outpatient basis; or
-
[CMS has] determined that the procedure can be appropriately and safely performed in an [Ambulatory Surgery Center (ASC)] and is on the list of approved ASC procedures or proposed by us for addition to the ASC list.ix
Not all criteria need to be met for CMS to determine that a procedure may be appropriately removed from the IPO list.
B. CMS Moves Towards Complete Elimination of the IPO List
In its Calendar Year 2021 Hospital Outpatient Prospective Payment Systems and Medicare Ambulatory Surgical Center Final Rule (CY 2021 OPPS/ASC Final Rule), CMS finalized a proposal to eliminate entirely its IPO list incrementally over a three-year period, beginning with 298 codes (including 266 musculoskeletal-related procedures).x Because CMS determined to eliminate the IPO list entirely, CMS’ criteria to evaluate whether to remove procedures from the IPO list were not applied to the 298 codes removed.xi CMS concluded that the IPO list was no longer necessary due to the evolving nature of the practice of medicine, which had allowed more procedures to have a shorter recovery time supporting coverage on an outpatient basis. In addition, CMS rationalized that physicians’ clinical judgment, state and local licensure requirements, accreditation requirements, hospital conditions of participation (CoPs), medical malpractice laws, and CMS quality initiatives provided sufficient guardrails to ensure that patient safety would not be compromised in the absence of an IPO list. CMS acknowledged that the difference between the need for inpatient care and the appropriateness of outpatient care had become less distinct.xii
C. CMS Reverses Course, Halting (for Now) Elimination of the IPO List
In its CY 2022 OPPS/ASC Final Rule, CMS decided to halt the elimination of the IPO list, and, after applying its criteria to evaluate whether to remove procedures from the IPO list, CMS determined to return the majority of the 298 procedures removed from the IPO list in CY 2021 to the IPO list beginning in CY 2022 (except for CPT codes 22630 (Lumbar spine fusion), 23472 (Reconstruct shoulder joint), 27702 (Reconstruct ankle joint) and their corresponding anesthesia codes).xiii CMS also finalized a proposal to codify its criteria for determining whether a procedure should be removed from the IPO list in a new 42 C.F.R. §419.23.xiv
In making these decisions, CMS acknowledged that providers needed more time to adjust to the removal of so many procedures from the IPO list.xv To properly prepare for the elimination of the IPO list, providers needed more time to develop patient selection criteria and other protocols to identify whether a procedure can be safely provided in the hospital outpatient setting.xvi CMS reiterated that “the removal of a particular procedure from the IPO list does not require that all beneficiaries be treated in the outpatient setting.” Because procedures removed from the IPO list may be appropriately performed in both the hospital outpatient and inpatient settings, physicians and clinical care teams must “exercise complex medical judgment to determine the appropriate setting of care in accordance with the two-midnight rule.”xvii
CMS sought comment on whether it ought to maintain a long-term objective of eliminating the IPO list, or whether it should be maintained and systemically scaled back in accordance with applicable standards of practice.xviii
D. Importance of the Two Midnight Rule
The two-midnight rule is codified at 42 C.F.R. § 412.3 (d)xix and is the regulatory criteria for inpatient hospital admissions.xx Under the two-midnight rule, unless an exception applies, an inpatient hospital admission is generally appropriate where the admitting physician expects a patient to require hospital care that will cross two midnights. There are two regulatory exceptions to this general rule: (1) Inpatient hospital admissions for patients undergoing procedures on the IPO list; and (2) Inpatient hospital admissions for patients expected to require hospital care that will cross less than two midnights but nonetheless require inpatient care (oftentimes referred to as the case-by-case physician judgment exception).xxi
In the CY 2022 OPPS/ASC Final Rule, CMS summarized the following:
Regardless of the status of the IPO list, we believe that the 2-Midnight benchmark remains an important metric to help guide when Part A payment for inpatient hospital admissions is appropriate. As technology advances and more services may be safely performed in the hospital outpatient setting and paid under the OPPS, it is increasingly important for physicians to exercise their clinical judgment in determining the generally appropriate clinical setting for their patient to receive a procedure, whether that be as an inpatient or on an outpatient basis. Importantly, removal of a service from the IPO list has never meant that a beneficiary cannot receive the service as a hospital inpatient—as always, the physician should use his or her complex medical judgment to determine the appropriate setting on a case by case basis.
As stated previously, our current policy regarding IPO list procedures is that they are appropriate for inpatient hospital admission and payment under Medicare Part A regardless of the expected length of stay. Halting the elimination of the IPO list would mean that this will remain true for all services that are still on the list. As in previous years, any services that are removed from the list in the future will be subject to the 2-Midnight benchmark and 2-Midnight presumption. This means that for services removed from the IPO list, under the 2-Midnight presumption, inpatient hospital claims with lengths of stay greater than 2 midnights after admission will be presumed to be appropriate for Medicare Part A payment and will not be the focus of medical review efforts, absent evidence of systematic gaming, abuse, or delays in the provision of care in an attempt to qualify for the 2-Midnight presumption. Additionally, under the 2-Midnight benchmark, services formerly on the IPO list will be generally considered appropriate for inpatient hospital admission and payment under Medicare Part A when the medical record supports either the admitting physician’s reasonable expectation that the patient will require a stay that crosses at least 2 midnights, or the physician’s determination that the patient required inpatient hospital care despite an expectation of a shorter length of stay.xxii
Complicating the analysis for hospitals, CMS does not recognize a difference in the intensity of services performed in the inpatient hospital or outpatient hospital “settings.” In issuing the two-midnight rule, CMS explained, “we do not refer to ‘level of care’ in guidance regarding hospital inpatient admission decisions. Rather, we have consistently provided physicians with [a] time-based admission framework to effectuate appropriate inpatient hospital admission decisions.”xxiii The distinction between inpatient hospital care and outpatient hospital care is one of reimbursement. Regardless of whether a procedure is performed in the inpatient or outpatient “setting,” there should be no relative difference in the safety of a procedure performed in the hospital. From a compliance perspective, to mitigate potential audit risk, hospitals may choose to take a conservative position and admit a Medicare beneficiary as an inpatient to undergo a procedure formerly on the IPO list only if the admitting practitioner expects the beneficiary to require two midnights or more of hospital care and treat other beneficiaries on an outpatient basis.
E. Medical Review of Procedures Removed from the IPO List
When procedures are removed from the IPO list, providers oftentimes struggle to determine the proper status to assign patients undergoing the procedures (i.e., inpatient versus outpatient). In order to assuage provider concerns related to audit risk related to assigning patients with improper status,xxiv over time CMS has implemented various medical review exemptions for procedures removed from the IPO list:
- In its CY 2020 OPPS/ASC Final Rule, CMS finalized a policy to exempt procedures that had been removed from the IPO list from reimbursement denials based on patient status determinations for two calendar years following their removal from the IPO list. During this time:
- Although the Beneficiary and Family-Centered Care Quality Improvement Organization (BFCC-QIO) (i.e., the contractor assigned to perform most patient status reviews)xxv was permitted to review these claims, it was not permitted to deny payment based on the patient’s status/setting of care (i.e., inpatient versus outpatient).
- Instead, the BFCC-QIO was tasked to provide education related to compliance with the two-midnight rule for such claims.
-
The BFCC-QIO was prohibited from referring providers to the recovery auditors (RACs) for noncompliance with the two-midnight rule based on its reviews of such claims, and the RACs were prohibited from reviewing such claims for patient status.xxvi
-
In its CY 2021 OPPS/ASC Final Rule, CMS expanded its exemption of medical review for claims removed from the IPO list on or after January 1, 2021 indefinitely, i.e., until such time as CMS acquired data to indicate the procedure was performed more commonly in the outpatient setting than in the inpatient setting. This expanded exemption period was thought to be necessary to allow providers to adjust to the 298 services removed from the IPO list.xxvii
-
In its CY 2022 OPPS/ASC Final Rule, because CMS proposed to halt the elimination of the IPO list and return the services removed from the IPO list in CY 2021, it determined that an indefinite exemption period was no longer warranted. CMS returned to its two-year exemption and codified this exemption at 42 C.F.R. § 412.3 (previously, medical review exemptions were issued on a sub-regulatory basis).xxviii
III. Conclusion
Future rulemaking will determine whether CMS will maintain its longer-term objective of eliminating the IPO list entirely, or whether it will systemically scale back the IPO list as supported by standards of practice. With the return of most procedures eliminated from the IPO list in 2021 effective January 1, 2022, hospitals that implemented processes to perform certain procedures removed from the IPO list on an outpatient basis need to ensure that clinicians are educated that these procedures have returned to the IPO list, as procedures on the IPO list will be reimbursed only if the service is performed in the inpatient setting.xxix
Jessica L. Gustafson and Abby Pendleton are founding shareholders of The Health Law Partners, P.C., in Farmington Hills, MI
(The references for this article are extensive - Please email Dr Hirsch at signaturedoc@gmail.com for the list if needed).
|
|
|
|
Yes, You Can Admit Psychiatric Cases as Inpatients
|
Carolyn Dutton, MD, FACP, FACEP, CHCQM-PHYADV
ACPA Board Member, GAC Committee Co-Chair
|
|
Have you ever been told that you can’t admit a psychiatric patient to inpatient status in your hospital? Have you ever been told you are not a licensed psychiatric facility, or a psychiatrist, and therefore can't admit psychiatric patients as inpatients? Have you ever heard that inpatient psychiatric patients in an acute care hospital will be lower down on the priority transfer list to be discharged to an inpatient psychiatric hospital? These are common myths propagated in acute care hospitals. Patients with acute health problems often seek care through hospital emergency departments and this includes behavioral health. In 2016 there were nearly 10 million stays with a principal or secondary mental and substance use disorder diagnosis, constituting more than one in four inpatient stays according to the Agency for Healthcare Research and Quality.i Acute care hospitals can and are expected to provide emergent psychiatric stabilization.
Status determination can play a role in the prioritization of patients transferring to an inpatient psychiatric hospital. Consult your compliance team and organizational policy as well as state guidelines regarding the effect of status on transfer in your region. Depending on your geographic location, emergency department patients and observation patients may take priority over inpatients.
CMS has specific guidelines regarding the delivery of psychiatric services at inpatient psychiatric facilities (IPF) which are distinctly different from stabilization care provided at acute care hospitals.ii These services include psychiatrist supervision and multidisciplinary teams providing psychological services, social services, psychiatric nursing, and therapeutic activities.iii There are also specific staffing requirements for a psychiatric unit to ensure adequate numbers of qualified professional and supportive staff available to formulate written individualized comprehensive treatment plans which are beyond the scope of acute care hospitals.
Since October 1, 1983 most hospitals, excluding rehabilitation, psychiatric, children, cancer, long term care, rehab and psychiatric distinct units within the hospital have been paid under the inpatient prospective payment system (IPPS).iv The IPF prospective payment system (PPS) responsible for paying psychiatric hospitals calculates a standardized federal per diem rate paid to all IPFs based on the sum of the national average routine operating, ancillary, and capital costs for each patient day of psychiatric care in an inpatient psychiatric facility. This is adjusted for patient age, MS-DRG, and selected comorbidity categories. It includes adjustment for wage index, location, and outliers like the IPPS.
Implemented in 2005, Section 124 of the Balanced Budget Refinement Act of 1999 (BBRA) required that a per diem PPS be developed for payment made for inpatient psychiatric services furnished in psychiatric hospitals and psychiatric units of acute care hospitals and critical access hospitals. Certain coverage requirements must be met for Medicare to pay for inpatient psychiatric services under the IPF PPS; patient characteristics include Medicare Severity Diagnosis Related Group (MS-DRG) classification, age, presence of specified comorbidities, and length of stay.v
Payment is made under the IPF PPS for claims with a principal diagnosis included in Chapter Five of the International Classification of Diseases (ICD-9- or ICD-10 as applicable) or the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition, Text Revision (DSM-IV-TR). Absent acute medical conditions, patients hospitalized in acute care hospitals generally fall under the Major Diagnostic Category (MDC) 19 classification of Mental Diseases and Disorders. Listed are a few of the commonly seen principal diagnoses which group to the specific MS-DRG.
876: OR procedure with principal diagnosis of mental illness
880: Acute adjustment Reaction and Psychosocial dysfunction (delirium, conversion disorder)
881: Depressive Neuroses (major depressive disorder, postpartum depression)
882: Neuroses except depressive (post-traumatic stress disorder, somatization disorder)
883: Disorders of personality and impulse control (paranoid personality disorder)
884: Organic disturbances and intellectual disability (vascular and unspecified dementia)
885: Psychoses (schizophrenia, bipolar disorder, manic episode)
886: Behavioral and developmental disorders (impulse and conduct disorder)
887: other mental disorder diagnoses (eating disorder)
Providers need to ensure that they are giving specificity for psychiatric diagnoses. Dr. Erica Remer, Co-Chair of the ACPA Clinical Documentation Integrity Committee notes “specificity of depression could be the difference between landing in DRG 881 Neuroses (RW 0.8020) or 885 Psychoses (RW 1.2394), and if a mood disorder is due to some other known physiological condition, it may end up in 884 (RW 1.4473). Specificity, especially for depression and bipolar disorders, consists of single episode vs. recurrent episodes and severity of current or most recent episode, including the presence of psychotic features. As a secondary diagnosis, if a patient is in partial or full remission, that should be noted as well.”
Note that both acute care hospitals and inpatient psychiatric facilities use the same MS-DRG classification system. Place of service on the UB-04 differentiates patient location. Now that we have established that you can admit patients with acute psychiatric conditions to an acute care hospital and bill accordingly, I defer you to the two-midnight rule for status determination. Regarding Medicare Advantage or Part C plans, I remind you that “In the United States, according to federal law, Part C providers must provide their beneficiaries with all services and supplies that Original Medicare Parts A and B cover.”vi
|
|
|
|
Can a Patient with Sepsis Be Discharged from the ED? |
Erica E. Remer, MD, FACEP, CCDS
Member, ACPA Board of Directors
Co-Chair, ACPA Clinical Documentation Integrity Committee
|
|
There has been a lively debate on LinkedIn regarding an article which came out in JAMA Open Network February 10, 2022 called Prevalence, Characteristics, and Outcomes of Emergency Department Discharge Among Patients With Sepsis, by Peltan, et. al., instigated by Dr. Ronald Hirsch and stoked by me. Dr. Cesar Limjoco posted a meme that says, “Clinical Truth: One dose of antibiotics in the ED resolves sepsis only when it isn’t sepsis,” attributed to Dr. Ryan Greiner who is a System Medical Director and Physician Advisor, and I wholeheartedly agreed.
Ron contacted the author of the original article informing them of our discussion, and we were referred back to a commentary which had been published with the manuscript, entitled, Elucidating the Spectrum of Disease Severity Encompassed by Sepsis, by C. Rhee and M. Klompas (both MDs and MPHs). I strongly encourage you all to read both the original article and this companion piece.
The original article stated that 16% of patients who “met sepsis criteria” were discharged from the ED, and 66% of those had urinary tract infections. The 30-day mortality for this cohort was 0.9% as opposed to 8.3% for patients admitted to the hospital. I was unable to ascertain which organ dysfunction was present in this group of patients (e.g., infection correlated with organ dysfunction). There is a graphic in the supplemental materials which demonstrates that patients who were admitted had higher increases in SOFA components than those discharged.
The article which elicited this commentary starts off referring to it as "sepsis syndrome." Although they are probably hailing back to the days when we thought there was sepsis, severe sepsis, and septic shock on a spectrum, there is no way to code "sepsis syndrome." I refer to sepsis as the condition formerly known as "severe sepsis." All diagnoses of sepsis now should have an additional code of R65.20/1, (Severe sepsis without/with shock), which can only be captured if the documentation supports it.
Coders are permitted to capture "severe sepsis" if the clinician specifies that the organ dysfunction is sepsis related. The macro that I recommend is: Sepsis due to [infection] with acute sepsis-related organ dysfunction as evidenced by [organ dysfunction/s]. This serves multiple purposes. First, it ensures there is a bona fide infection. Second, the patient must have organ dysfunction (not just deranged vital signs). Finally, the linkage of acute sepsis-related with organ dysfunction gives the coder permission to pick up R65.20.
I think this also highlights the problem with this study. The way they identified patients is if body fluid cultures were obtained and antibiotics were administered, indicating an infection (prophylaxis and empiric antibiotic administration were excluded). Then, they reviewed the chart and determined if there was organ dysfunction as per SOFA compared to baseline according to labs. One of the authors told me in a personal communication that, “We did not use discharge diagnosis or clinical documentation.” I am relieved that they used organ dysfunction as opposed to SIRS, however!
The Third International Consensus (Sepsis-3) clearly stipulates that there are no gold-standard diagnostic tests, and that sepsis is a clinical diagnosis. Organ dysfunction must be associated with the sepsis. Underlying infection (e.g., pneumonia causing hypoxemia), dehydration, other conditions like Gilbert’s disease can cause derangement of the components of the SOFA score. Infection plus organ dysfunction isn’t sepsis; infection plus sepsis-related organ dysfunction is. If the provider hasn’t made the call of sepsis and the researcher isn’t reviewing the clinical documentation, then how do they know whether the organ dysfunction was sepsis-related or not?
We old-timers know that inherent to the diagnosis of sepsis, which is a clinical diagnosis without any gold standard diagnostic criteria, is the fact that the patient is SICK. Sepsis-2 was an attempt to facilitate clinicians to not miss the diagnosis of sepsis because it has a high mortality (just the disparate 30-day mortality rates, 0.9% vs. 8.3%, makes one question whether the discharged population really had sepsis). It was determined that too wide a net was being cast, so Sepsis-3 tried to identify the essence of what indicated a patient was SICK, hence, mandating acute organ dysfunction. When I teach, I explain that "sepsis without organ dysfunction" is called... "pneumonia" or "UTI" or "cellulitis."
The problem with data is that the output is only as good as the person drawing the conclusion. Is the clinician ticking SOFA boxes without considering whether a dysregulated host response to infection caused the derangement? Is hypoxemia from the pneumonia itself or is it sepsis-related? Is a bump in creatinine in a UTI from the localized infection, dehydration, or from resultant sepsis?
I think this study really demonstrated that patients with infection who are sent home from the emergency department are not as sick as patients who are admitted to the hospital. That’s good. I agree with the commentators that “the most important reason to call an infection sepsis is to emphasize the severity of the condition and trigger immediate aggressive care.”
Perhaps we would benefit from reintroducing the criterion for a patient to appear SICK in order to consider a diagnosis of sepsis. I don't believe that we want to impose a threshold duration of organ dysfunction, as has been suggested. We may benefit from insisting there needs to be organ dysfunction not involving the infected organ/system.
There are payors who won't acknowledge the possibility that sepsis can be placed in Observation status. How common is it really (or should it be) to have a patient with genuine sepsis discharged to home from the ED? It should be about as common as it is to bill Critical Care Time in the ED for a discharged patient - it happens, but it is rare.
I agree with Dr. Ryan Greiner, a system medical director and physician advisor, who said, "One dose of antibiotics in the ED resolves sepsis only when it isn't sepsis."
References
Dr. Remer is the founder and president of Erica Remer, MD, Inc., icd10md.com.
|
|
American College of Physician Advisors
President's Corner
|
|
It is truly surreal that we have entered into the third year of life with COVID-19. After an initial 12 months of horror and fear and a second year of hope and optimism (not to mention more desperation and feeling overwhelmed), you might be experiencing this third year like I am – obsessing over getting back to business. Not to say anyone has been slacking – absolutely not! But, I think we can all recognize a number of different areas where strategic planning or incremental progress toward a goal came to a standstill due to the pressures of the pandemic.
One example that’s likely pretty universal across the country in health systems large and small is the Observation Unit. The initial onslaught of COVID-19 followed by the Delta and then Omicron variants and then a cascade of non-COVID patients hospitalized with chronic conditions made worse by staying away from health care, seems to have perpetually kept our hospitals full. With stories of Emergency Departments boarding dozens of patients at a time in their hallways and hospitalized patients who are ready to discharge but have no accepting facility to take them, it’s not surprising that Observation Units everywhere dissolved into general medical/surgical units.
Perhaps your Observation Unit is filled with patients in Inpatient status. Maybe you’ve sustained a functional loss of the ability to prioritize testing and imaging for patients in Outpatient status with Observation services. Or, how about provider staffing? If, pre-pandemic, you had a dedicated hospitalist team covering the “OBS patients” on the “OBS Unit,” chances are that geographical dedication went out the window when the census increased exponentially. We at the American College of Physician Advisors would like to help!
Thursday evening, March 3rd, our Observation Committee – led by Drs. Bernard Ravitz, Anuja Mohla, and Amit Wadhwa – will host their second Town Hall. (If you are reading this after 3/03, not to worry! Details will be coming soon about how you can watch the recording.) This event will focus on the pros and cons of different models and features of Observation Units including an overview of existing best practices. The forum is free of charge and open to anyone who wishes to register. It is intended not only for physician advisors, but also colleagues in Utilization Review, Case Management, Revenue Cycle, and other hospital and health system leaders. At the time of registration, you will have an opportunity to submit questions for the panel. Participants will also be able to ask questions in real time during the event. This is a great opportunity to learn from the ACPA Observation Committee and your colleagues from across the country! I hope to see you there.
|
|
Juliet B. Ugarte Hopkins, MD, CHCQM-PHYADV
(Pronouns: She/Her)
President, ACPA
Dr. Juliet B. Ugarte Hopkins is Physician Advisor for Case Management, Utilization, and Clinical Documentation for ProHealth Care, Inc. in Waukesha, WI.
|
|
The American College of Physician Advisors (ACPA) publishes and distributes materials created by our members and speakers for the benefit of all ACPA members. ACPA does not certify the accuracy or authority of these materials. These materials are distributed and presented as research information to be used by ACPA members, in conjunction with other research deemed necessary, in the exercise of ACPA members’ independent professional judgment. Original and fully-current sources of authority should be researched by ACPA members. ACPA disclaims all liability in relation to reliance on the content of these materials. The views expressed in the materials are the views of the material's authors and do not represent the views of ACPA. Any references are provided for informational purposes only and do not constitute endorsement of any sources. |
|
|
|
|
|
|