March 27, 2020
The Out-of-Pocket Health News Digest:
Poverty and Health Special Edition
|
|
Below you will find briefs about recent health policy news stories. With this special edition, our hope is for students to understand some of the ways that poverty connects to health, and how policy decisions impact vulnerable populations.
This compilation is produced by the HPSA Education Committee: Sharoni Bandyopadhyay, Matthew Dunn, Payton Watt and Courtney Zott.
|
|
The Connection Between Housing Policy and Health Policy
|
|
Society often views homelessness as a burden and a public policy issue, and less frequently as one that could be impacted by health policy. Although some experts see the clear connection between health and homelessness, there has not been enough policy progress in this area.
Not having stable housing or environmentally safe housing leads to detrimental health outcomes that cause an increase in health care utilization. On any given night in 2018, there were approximately
500,000 individuals experiencing homelessness
in the United States. Individuals experiencing homelessness have
higher rates of diabetes, hypertension, respiratory illness, food insecurity
, and more. They are also
three times more likely to utilize the emergency department
in any given year compared to the general population. Moreover, in 2015 about 39 million Americans
paid more than 30% of their income on housing
, which is the
threshold
to be considered affordable. Of individuals living in poor-kept housing, they are likely exposed to
higher levels of lead, radon, pests, and mold
, which can lead to higher levels of asthma, allergies, and serious health conditions.
The best solution to addressing homelessness and inadequate housing conditions is offering high-quality affordable housing. When Portland, Oregon
built more affordable housing
they saw a decrease in Medicaid expenditures by 12%, a decrease in emergency department utilization by 18%, and an increase in primary care by 20%. Regardless, there are many ongoing debates as to what the health system’s role should be in addressing social determinants of health, including housing. Advocates suggest that state Medicaid programs could support health systems in providing housing-related services; health systems could invest in housing stock, create partnerships with housing non-profits, or
use their community benefit dollars to build adequate affordable housing
. These will all become increasingly important considerations as
housing prices continue to rise much more quickly than wages
.
|
|
The Intersection of Poverty, Incarceration, and Health
|
|
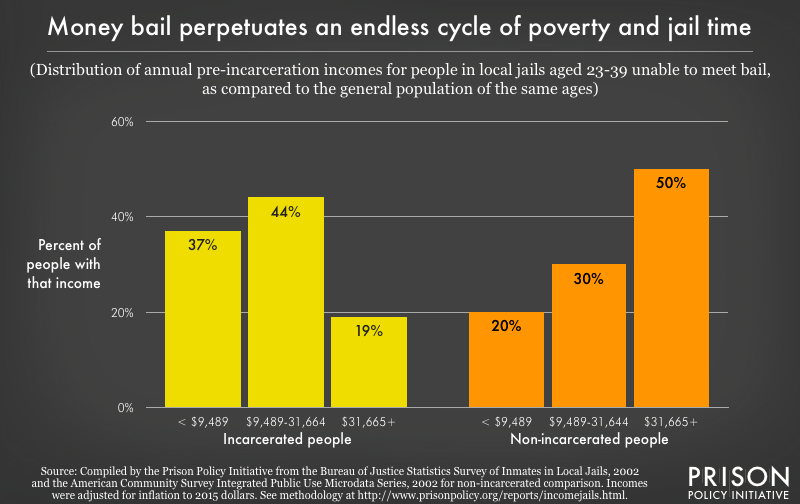
The criminal justice system has a profound impact on public health. In the United States, people are incarcerated at a greater rate than any other country:
698 per 100,000 residents
as of March 2020. Furthermore, the process by which individuals navigate the system is marred with injustice and inequity, including on the basis of wealth and income. For instance, there are over 550,000 Americans without a charge or conviction locked in local jails and other facilities, because they cannot afford the bail for release. Among individuals detained before their trials, the median annual income for men is $15,598 and $11,071 for women,
according to a 2016 report
. This is significantly less income compared to those who are not detained pre-trial.
Research has shown a strong link between mass incarceration and health. While in prison or jail, many Americans experience
unsafe and inhumane
living conditions, such as physical abuse, solitary confinement, and exposure to infectious diseases. Studies consistently find
a spike in mortality rates
among those recently released from confinement. Long-term effects of incarceration are more difficult to measure, but studies have found higher rates of premature mortality and chronic mental health challenges.
Criminal justice advocates and experts have their sights set on a number of reforms to this system. Professor Rachel Barkow at the NYU School of Law argues the single most important change would be to get rid of
mandatory minimum
requirements, which often lead to excessive punishments and create additional racial disparities in sentencing. Some cities, including Philadelphia, have
abolished cash bail
for low-level charges so that poor individuals are not disproportionately detained while waiting for trial. Finally, although many proposed reforms will face resistance in the legislative process, executive authority over clemency is a powerful tool and can be used to combat mass incarceration. The president can issue pardons for federal offenses, and governors can issue pardons for state-level offenses
|
|
How Income Impacts Access to Health Care
|
|
The disparities in life expectancy between high- and low-income individuals in the U.S. are stark. The top 5% of earners have seen their life expectancy increase by 2.5 years since 2001, while those in the bottom 5% have seen no gains. Additionally, men and women in the bottom 1% of earners live 15 and 10 years fewer respectively than their counterparts in the top 1%.
Part of this gap has to do with underlying disparities in access to health care. Low-income individuals are less likely to be insured despite the ameliorating effects of the Affordable Care Act, as they are less likely to work for an employer that offers health benefits or earn enough income to afford coverage offered by their employer or on the exchanges. Additionally, low-income adults do not qualify for Medicaid in the 13 U.S. states that chose not to expand their programs (Alabama, Florida, Georgia, Kansas, Mississippi, Missouri, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, and Wyoming). Meanwhile, the rate of people who are underinsured - people whose out-of-pocket costs make up a high portion of their income - has been rising since the passage of the ACA, in part due to actions weakening the law since its passage. Lack of adequate insurance increases the likelihood that an individual does not have a regular care source, does not receive needed care for chronic conditions or even more acute health conditions, does not receive needed services or medications for mental health conditions, or forgoes care due to cost.
Medicare-for-All and other proposals for universal health care are an attempt to address disparities in access to care by untethering health insurance in the U.S. from income, as most of the country’s peer nations do in the Organisation for Economic Cooperation and Development. However, there is significant resistance from the hospital and health insurance industry, as well as from elected officials in both political parties.
|
|
State-level Innovations to Address Social Determinants of Health
|
|
Medicaid
provides insurance coverage to 75 million low-income Americans, making it the primary source of coverage for those living in poverty. Because Medicaid is administered on the state-level, the program can serve as a bridge between federal regulations and community-based resources. Individual states can apply to exempt CMS regulations and implement innovative approaches to coverage through
Section 1155 Medicaid demonstration waivers
.
These waivers allow the State to utilize the funds provided for Medicaid and CHIP in experimental ways to test out new payment models, coverage of services or eligibility requirements.
Several of these innovations experiment with addressing SDOH in an effort to address the underlying factors which further contribute to poor health outcomes among those of low socioeconomic status, such as housing, transportation and food access. States often outline these objectives to improve population health through their
managed care contracts or value-based purchasing contracts
.
Through managed care organizations (MCO) contracts, accountable care organizations (ACO) contracts, or general contracting guidelines, states can dictate which SDOH need to be addressed; incorporate SDOH into contracting agreements; and outline how these interventions will be monitored and reimbursed by the state.
Some interventions that may be defined in contracts include alternative payment models, payment incentives, or reimbursement for non-traditional services. Alternative payment models can include allocating funding to MCOs to address housing services or food security. Likewise, payment incentives, such as value-based purchasing, can reward health plans for meeting certain quality metrics for maternal mortality or lead levels in blood for children, which are often common in impoverished communities. These incentives encourage health plans to implement screenings and address SDOH through providing financial rewards. Medicaid can also encourage MCOs to provide extra services: “in-lieu of” services or “value-added” services. “In-lieu of” services substitute for a different service that is usually covered under MCOs, such as a home visit for pregnant mothers instead of a prenatal visit. “Value-added” services include additional services like a nutrition class. These provide flexibility to health plans in addressing social needs.
|
|
|
|
|
|
|