The public health emergency (PHE) was set to expire on October 18, 2021. Secretary Becerra has once again renewed this PHE for a period of 90 days, which will extend the coverage for telephone-only services until at least January 17, 2022. Currently, it is expected that HHS will continue to renew its declaration of the PHE every 90 days through the end of 2021 and will provide 60 days’ notice prior to ending it.
Telephone-only services were scheduled to be extended for mental health services only. However, ASIPP has been working on making telephone-only services permanent to provide appropriate care for our chronic pain patients. Consequently, all other telemedicine services (with audio and video) have been considered in the fee schedule and are expected to last until December 2023 while collecting the data.
Once again, the Biden administration promised that they would give providers at least 60-day notice prior to ending the PHE to avoid any confusion or operational issues. We should learn more in the next 30 days about a further extension of this PHE or the extension of telephone-only services in line with other services through the CMS final physician payment schedule which is due in November.
|
|
Your trusty cloth masks have gotten you through more than a year of pandemic. Heading into the winter, you might want an upgrade.
That's because some disposable masks — like surgical masks and KN95 masks — just plain work better, experts say. And plenty of them are available now, a turnaround from the beginning of the pandemic when the highest-quality masks needed to be reserved for healthcare professionals.
Your trusty cloth masks have gotten you through more than a year of pandemic. Heading into the winter, you might want an upgrade.
|
|
U.S. workers handed in nearly 20 million resignations this spring and summer
This year’s bold career move is walking out the door.
U.S. workers left their jobs nearly 20 million times between April and August this year, according to the latest federal data, a number more than 60% higher than the resignations handed in during the same period last year, and 12% above the spring and summer of 2019 when the job market was the hottest it had been in almost 50 years. The data doesn’t count retirements but includes people who have quit jobs for any number of reasons, such as taking a job elsewhere, going back to school, leaving to care of a family member or simply taking a break. The data also includes people who may have quit multiple times, for instance leaving a job on a college campus in May and then quitting a summer job in August.
Additional data from the Bureau of Labor Statistics shows a steady rise in the employed-to-employed rate, indicating that many people are switching jobs, not sitting on the sidelines. The U.S. labor force gained about 2 million employed people between April and August, though that level is still almost 3% lower than it was pre-pandemic.
|
|
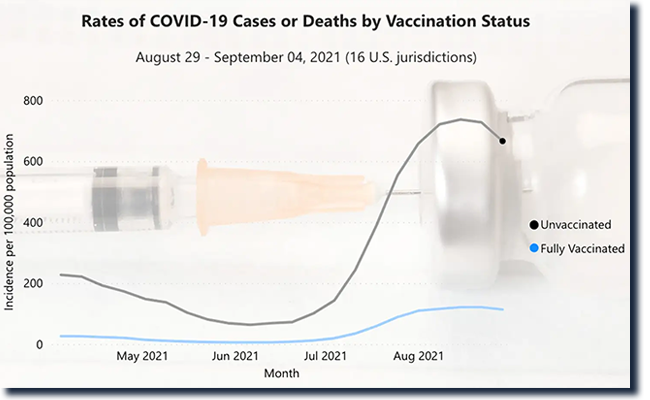
New tool also reveals numeric differences between vaccines
The CDC has begun to provide weekly data on COVID-19 cases and deaths by vaccination status, illustrating the stark differences between those who have received the shots and those who haven't -- and even revealing some differences between vaccines.
Users can parse the data by vaccine product, and while the unvaccinated have the highest rates of cases and deaths, there's a numeric divergence for the three vaccines as well.
Deaths among the unvaccinated peaked the week starting August 8, at 13.23 per 100,000 population, while deaths among those who had been vaccinated with one of the three products remained under four per 100,000 that week. For the vaccinated, deaths were numerically highest among Johnson & Johnson recipients, at 3.14 per 100,000, followed by Pfizer at 1.43, and Moderna at 0.73.
|
|
ASIPP® is pleased to offer a new feature for
its members to help provide value to you and your practice.
Click here to visit ASIPP®'s newly created site where you can
make purchases on our Amazon Store, learn more about and
join the ASIPP® GPO and ASIPP®’s partnership with
Fedora Billing & Revenue Cycle Management Company.
|
|
While not yet authorized, small trials suggest some booster combinations are not only safe, they may yield better protection.
Can someone get their initial COVID-19 vaccine from one manufacturer and then get a booster from another? The question has intrigued medical professionals since before the first shot went into an arm—and it’s far more than an academic issue. Allowing people to mix and match COVID-19 shots could significantly improve vaccine distribution and may even offer some medical benefits.
If the FDA eventually endorses mixing brands, the decision could help nationwide vaccination efforts, says Pedro Piedra, professor of molecular virology, microbiology, and pediatrics at Baylor College of Medicine in Houston. “At any time, a pharmaceutical company can have a manufacturing issue, whether that’s a contamination problem or a shortage of a reagent, so it’s helpful to have options,” he says.
|
|
The US Preventive Services Task Force is considering making several changes to its guidance on taking a daily aspirin to prevent heart disease and stroke.
On Tuesday, the task force posted a draft statement recommending that adults ages 40 to 59 who are at a higher risk for cardiovascular disease -- but do not have a history of the disease -- decide with their clinician whether to start taking aspirin, based on their individual circumstances.
This is the first time the task force has recommended that adults in their 40s talk to their doctors about whether to take aspirin for heart health.
|
|
Pain Medicine Case Reports (PMCR) and Editor-in-Chief Alaa Abd-Elsayed, MD, PhD would like to invite you to submit case reports and case series to the PMCR journal. Your article will be published free of charge.
Open access journals are freely available online for immediate worldwide open access to the full text of published articles. There is no subscription fee for open access journals. Open access journals are no different from traditional subscription-based journals: they undergo the same peer-review and quality control as any other scholarly journal.
Interested in becoming a member of the PMCR Editorial Board?
Editorial board members are asked to review 2-6 manuscripts per year. Please submit your most up-to-date CV to sgold@asipp.org for consideration.
For more information or to submit your articles, click here.
|
|
| CASE REPORT |
Nian Zhou, PhD, Xin Lin, BD, Xiaojun Zhang, PhD, Wei Jiang, PhD,
Jieliang Shen, PhD, Xiuming Guo, MD, PhD, Zhenming Hu, MD, PhD,
and Jie Hao, MD, PhD
Abstract
Background: Spondylolysis is a bony defect of the pars interarticularis that most commonly occurs in the lower lumbar spine. However, the condition is rare in the mid-lumbar region. Here, we report on a new technique that involves the use of a U-rod and pedicle screw with iliac bone grafting for the direct intrasegmental repair of mid-lumbar spondylolysis in a teenager.
Case Report: A 17-year-old male presented with complaints of mild low back pain after physical exercise, and the pain had aggravated in the last 3 months. Magnetic resonance imaging did not show compression of the intracanal neural tissue, and the lumbar discs did not demonstrate any obvious degeneration. He was diagnosed with L3 spondylolysis and lumbar sacralization. U-rod and screw construct with iliac bone grafting were used to directly repair the spondylolysis in L3. The low back pain totally disappeared 3 months after the surgery. A computerized tomography scan revealed the normal structure of L3 2 years post-surgically, and the internal fixation was removed 3 years later.
Conclusion: This novel technique involving the use of a U-rod and pedicle screw associated with iliac bone grafting for the direct repair of mid-lumbar spondylolysis in the teenager yielded a satisfactory outcome, which was confirmed by favorable clinical and radiographic outcomes after 3 years.
Key words: Mid-lumber spondylolysis, U-rod, direct repair
|
|
| HEALTH SERVICES RESEARCH |
Laxmaiah Manchikanti, MD, Sri Harsha Vardhan Senapathi, MD,
James M. Milburn, MD, Allan L. Brook, MD, Brahma Prasad Vangala, MBBS, Vidyasagar Pampati, MSc, Mahendra R. Sanapati, MD,
and Joshua A. Hirsch, MD
Abstract
Background: Despite the high prevalence of vertebral compression fractures (VCFs) associated with refractory pain, deformity, or progressive neurological symptoms, minimally invasive vertebral augmentation procedures, including vertebroplasty and kyphoplasty, have been declining in their relative utilization, along with expenditures.
Objectives: This investigation was undertaken to assess utilization and expenditures for vertebral augmentation procedures, including vertebroplasty and kyphoplasty, in the fee-for-service (FFS) Medicare population from 2009 to 2018.
|
|
| SYSTEMATIC REVIEW |
Laxmaiah Manchikanti, MD, Emilija Knezevic,
Nebojsa Nick Knezevic, MD, PhD, Brahma Prasad Vangala, MBBS, Mahendra R. Sanapati, MD, Srinivasa Thota, MD, Salahadin Abdi, MD, PhD, Alaa Abd-Elsayed, MD, Alan D. Kaye, MD, PhD, and Joshua A. Hirsch, MD
Abstract
Background: The Best Practices in Pain Management from the U.S. Department of Health and Human Services (HHS) describes interventional techniques as part of a continuum. Epidural injections are commonly utilized modalities in managing low back and lower extremity pain. Epidural injections were initially administered in 1901 where the first descriptions of caudal epidural with local anesthetic for low back pain appeared. Since then, multiple developments have occurred. Currently, epidural injections are provided by caudal, interlaminar, and transforaminal approaches. The comparative effectiveness of each modality has been studied. However, comparative assessment has been sparse.
Objectives: To assess the efficacy of 3 routes of administration of epidural injections for lumbar disc herniation.
|
|
Since this malpractice insurance program officially launched in November 2018, ASIPP has signed up hundreds of providers with an average savings of 30%. This is professional liability insurance tailored to our specialty and will stand up for us and defend our practices.
Norcal Mutual is 'A' Rated by AM best and is license in all 50 states. To read a few important points to keep in mind about the program, including discounts, administrative defense, cyber coverage, aggressive claims handling, and complimentary award-winning risk management CME activities, click here.
|
|
ASIPP® is now offering our members the benefit of a unique revenue cycle management/ billing service. We have received a tremendous amount of interest in the ASIPP® billing and coding program.
Click here to learn more about the negotiated rate for practices and more!
|
ASIPP® has formed a partnership with Henry Schein and PedsPal, a national GPO that has a successful history of negotiating better prices on medical supplies and creating value-added services for the independent physician. Working with MedAssets, PedsPal provides excellent pricing on products like contrast media that alleviate some of the financial pressures you experience today.
|
|
up-to-date news related to you, your practice, and your patients!
|
|
|
|
|
|
|