|
The Quarterly Newsletter of the HHQI Underserved Populations (UP) Network
|
|
|
|
|
|
|
 |
|
Quarterly UP Network Webinar | July 19, 2018 | 2-3 p.m. ET
This webinar will discuss several common barriers and strategies home health agencies (HHAs) face that are serving patients in rural areas. Learn how two HHAs addressed barriers that affected delivery of care including patient and clinician issues. This activity has been submitted to the Alabama State Nurses Association (ASNA) for 1.25 hours of Nursing continuing education. ASNA is an accredited approver of the American Nurses Credentialing Center's Commission on Accreditation.
Register now
.
Featured Experts:
Renee Grisham, Director of Nursing
 Mississippi HomeCare of Eupora (MS) Mississippi HomeCare of Eupora (MS)
Diana Lecher, Director
Chadron Community Hospital and Health Service (NE)
|
Now Available: April 2018 UP Network Webinar Recording
Check out the Serving Racial & Ethnic Minority Populations UP webinar recording where Carol Jimenez, JD Deputy Director, Office of Minority Health U.S. Department of Health and Human Services presented information addressed the continued health disparities for racial and ethnic minorities and the need for accurate data collection. She also explained why the National Culturally and Linguistically Appropriate Services (CLAS) Standards in health and healthcare will assist to advance health equity, improve quality, and help eliminate health care disparities by establishing a blueprint for health and healthcare organizations. There are free nursing continuing education credits still available with the recording in HHQI University.
|
Save the Dates: 2018 UP Network Webinars
|
|
|
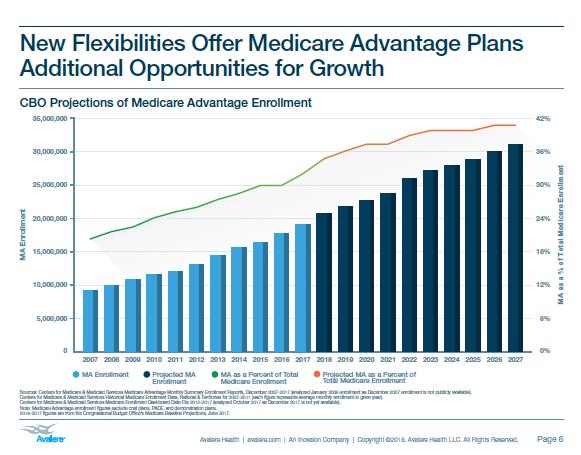
Medicare Advantage (MA) plans began in the 1970's offering an alternative to the Medicare Fee-for-Services (FFS) and continue to expand significantly across the country. Medicare beneficiaries who enroll in MA select a private health insurance plan. MA enrollment is projected to grow by 9% to 20.4 million in 2018, and Centers for Medicare & Medicaid Services (CMS) estimates that 34% of Medicare enrollees will be in a MA plans in 2018.
Home Health Agencies (HHAs) are providing care to higher percentages of MA patients than in the past. It is important to understand what services are available and more about this population in general to assist with improving outcomes and Home Health Star Ratings. The Quality of Patient Care Star Ratings
include Medicare and Medicaid, FFS and Advantage plans, for all the measures except for Acute Hospitalization, which is only
Medicare FFS from the claim-based data source.
Potential Changes in MA Patient Benefits
CMS pays the MA plan to provide beneficiaries the same health benefits of Medicare fee-for-service (FSS) health care services. MA plans can add additional options beyond the Medicare FSS plan. The plans now have more flexibility which will allow for more growth and services for beneficiaries. In April, CMS announced in a final rule to allow MA Plans to offer non-skilled in-home care services as a supplemental benefit beginning in 2019. The new definition will "allow supplemental benefits if they compensate for physical impairments, diminish the impact of injuries or health conditions, and/or reduce avoidable emergency room utilization" (CMS, 2018).
MA Plans could begin offering home-based palliative care in addition to personal supportive care. These services would assist HHAs financially to provide better care and improve quality of life for this underserved population.
|
In addition to the non-skilled in-home services, CMS also announced a proposal to allow MA plans to provide "primarily health-related" benefits. Currently some MAs already offer eyeglasses, hearing aids, dental care, and gym memberships. The new rule will allow plans to consider covering other needs that would improve the patient's health such as: transportation to medical appointments, air conditions for people with asthma, healthy groceries, grab bars, and daily aide care to assist with activities of daily living. Each plan will be able to decide the types of services that could be available and a determination process.
The new rule also includes more details on the lowering of drug prices for the Medicare prescription drug plan (Part D). Most MA plans offer Part D for beneficiaries. The focus for CMS' medication reduction includes:
- Allowing for certain low-cost generic drugs to be substituted onto plan formularies at any point during the year, so beneficiaries immediately benefit and have lower cost sharing.
- Increasing competition among plans by removing the requirement that certain Part D plans have to "meaningfully differ" from each other, making more plan options available.
- Increasing competition among pharmacies by clarifying the "any willing provider" requirement, to increase the number of pharmacy options that beneficiaries have.
(CMS, 2018)
The new changes should inspire more seniors to select MA plans over Medicare FFS. The Congressional Budget Office predicts continued growth - see Figure 1.
MA Plans and Disparities
CMS recently released the Racial, Ethnic, and Gender Disparities in Health Care in Medicare Advantage Report (April 2018). This report looks at MA data for 2015 and 2016. The report assesses 27 clinical care measures and 8 patient experience measures. Many of the clinical measures focus on access to care and medications, care coordination, specific disease management (e.g., blood pressure, COPD, diabetes, renal failure), BMIs, vision screening, avoiding potentially harmful medications in the elderly population, and behavioral health. Patient experience measures are also included and focus on access to care and timely medical appointments, customer service, accessing medications, and influenza vaccine.
CMS states in the report that as of 2016 the MA gender breakdown is:
O
verall, the quality of care received by women and men was similar, according to the report.
The MA racial/ethnic population breakdown is:
- 70% White
- 13% Hispanic
- 10% Black
- 4% Asian or Pacific Islanders
- 3% Multiracial
- < 0.5% were American Indians or Alaska Natives
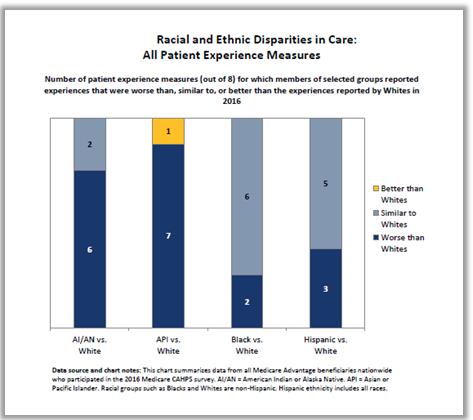
The report found, "with just one exception, MA beneficiaries in racial and ethnic minority groups reported experiences with care that were either worse than or similar to the experiences reported by White beneficiaries" - see Figure 2 (
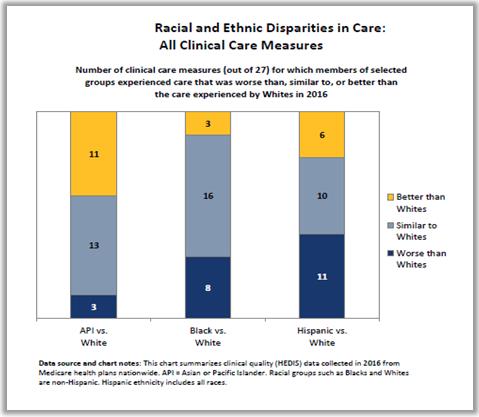
CMS, 2018). Racial and ethnic disparities were more variable for the clinical care measures than for the patient experience measures - See Figure 3.
Figure 2: Racial and Ethnic Disparities in Care: All Patient Experience Measures (CMS, April 2018).
Figure 3: Racial and Ethnic Disparities in Care: All Clinical Care Measures (CMS, April 2018)
The report provides background, breakdown for each of the measures in relationship to gender, racial/ethnic, and the combination of both aspects. This information may be useful to understand and improve outcomes for the MA population your agency is serving.
MA Performance Measures
HHAs should understand MA plan's purpose, goals, outcome/process measures, as well as services available to be able to partner more effectively to care for patients. CMS is beginning to be transparent with MA outcomes, satisfaction survey results, and other statistical information. CMS now provides information and Star Ratings on MA plans on www.medicare.gov for patients and families to compare plans including Medicare FFS.
The MA Star Ratings data comes from both patient satisfaction surveys and specific measures from the Healthcare Effectiveness Data and Information Set (HEDIS). The MA Star Measures focus on managing patient's care and are not assessing home health care. There are opportunities for HHAs to provide evidence-based practices to support improve patient outcomes, care coordination with the practitioners, and relationships with the plan. Some examples include:
- Annual Flu Vaccine
- Improving or Maintaining Physical Health
- Improving or Maintaining Mental Health
- The Plan Makes Sure Member Medication Records Are Up-to-Date After Hospital Discharge
- Managing Chronic (Long Term) Conditions (e.g., pain management, diabetes, blood pressure control, reducing the risk of falling, accurate medication list, readmission to a hospital within 30 days)
|
|
|
|
|
|
| This material was prepared by Quality Insights, the Medicare Quality Innovation Network-Quality Improvement Organization supporting the Home Health Quality Improvement National Campaign, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The views presented do not necessarily reflect CMS policy. Publication number 11SOW-WV-HH-ADL-061518 |
|
|
|