Community-acquired pneumonia facts
A recent review regarding strategies for triage and management of community acquired pneumonia in the
Cleveland Clinic Journal Of Medicine states that
in 2011 there were 915,500 episodes of community acquired pneumonia in adults at least 65 years of age. Medical costs in 2011 exceeded $10 billion. The National Center for Health Statistics reported in 2017 there were
1.7 million visits to the emergency room in which pneumonia is listed as the primary discharge diagnosis. From the same source
49,157 people had pneumonia listed as the cause of death in the US.
From a 2015 study quoted in this review it is notable that
only 38% of 2,200 actively cultured and tested individuals provided a definitive diagnosis. Blood and sputum bacterial cultures, nasopharyngeal or oropharyngeal swabs, and antigen testing were all used to identify a specific recognized pulmonary infection. Of the 38%, 25% (
clearly the majority) were viral infections. 14% were bacterial. 5% of viral infections were co-infected with a second virus or bacterial organism (dual infection).
I find it dismaying given this information that no new antiviral therapies to address have been developed. We can treat influenza with specific antiviral medication. We routinely hang antibiotics which only kill bacteria in hospitalized patients. Traditionally it is understood that antibiotics don't kill viruses.
We may learn from the recent COVID-19 story that one antibiotic commonly prescribed for community pneumonia including hospitalized patients may have antiviral effects. This medication is azithromycin, the famous "Z-pak". When taken in combination with hydrochloroquine it added significant improvement. This suggests it
may have antiviral properties to COVID-19 virus.
Covid-19 Clinical Characteristics
A
JAMA Original Investigation article reported on138 patients who had pneumonia from the novel coronavirus. The patients were admitted to Zhongnan Hospital of Wuhan University in Wuhan, China. This was a retrospective (look back) 28 day review starting January 1. The final date of follow up being February 3,2020.
This study reported patient demographics, symptoms, laboratory findings, x ray findings, treatment information and outcomes. The data showed some good test measurements that support the diagnosis and which can help predict severity of COVID disease. There were some distinguishing x-ray patterns as well. Patients who ended up in the ICU tended to have certain higher abnormal lab findings, abdominal pain and loss of appetite over the other COVID cases.
Very important information relates to what was defined as Hospital-associated transmission. There were 138 total cases. Forty of the 138 people infected were the hospital staff. That is 29% of total cases! An additional 17 (12.3%) of patient cases developed COVID in the hospital.
This means 41% of this patient group got infected in the hospital- over twice as many were health professionals and the rest were patients admitted for other things. 26% of infections resulted in ICU transfer for care. Of that group 41.7% went on a ventilator. Of the 138 cases, 6 died, demonstrating a case-study mortality of 4.3%.
Of the infected health care workers, the majority (77.5 %) worked on general wards,17.5% were emergency room department staff and
only 2 (5%) were Intensive Care Unit staff.
The inference to be made here (a take-home message) is that it is highly likely the ICU staff followed the proper/recommended Personal Protection Equipment use and protocols and this translated to a far lower infection transfer than the more relaxed protocols of a general ward. This factual information strongly supports the idea that hospital staff during this outbreak need to have optimal face and secretion precautions regardless of where in the hospital they work.
Another interesting tidbit in this group was one patient presented with abdominal pain (not an expected complaint) and was admitted to a general surgical floor. Case review suggests 10 workers and 4 of the patients on that floor were sickened by that initial surgically triaged case. The patient didn't have a surgical disease but a surgical problem was suspected due to the abdominal pain complaint. Hospital staff should not assume that a patient admitted for possible surgical pain is not infected with COVID-19. This triage case resulted in 14 other persons getting the virus.
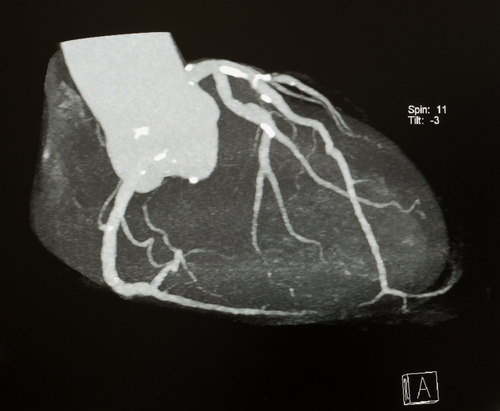
An Argument for CT Coronary Calcium Score As a Screening Test
|
|
| Coronary Plaque is Dense/Calcified |
When it comes to public health and screening, testing should be: available, safe, affordable and have predictive value for the disease in question. For the past 2-3 editions of the American Journal Of Medicine I have been seeing letters from the editors and now this most recent Commentary article which I feel offers a very compelling argument in favor of performing an imaging test to help identify high risk coronary disease persons in the general population.
The physician authors reference colorectal screening with colonoscopies as well accepted screening practice for preventing colon cancer. They point out this testing modality costs on average $3000 per test, involves a thorough bowel prep, one day of lost work and while tolerated it has significant side effects. As a baseline approximately 50,000 persons a year in the US die of colorectal cancer. They point out that the specialties of Gastroenterology and Cancer developed the screening recommendations as they learned that the natural history of colorectal cancer follows the development of advanced cancer. Mortality and morbidity of treating cancer is significant whereby removing polyps is a very simple and generally safe procedure and lowers the odds of cancer in the colon and rectum developing.
The logic for recommending CT calcium scores goes like this:
- 600,000 people a year die of coronary heart disease
- The presence of significant coronary calcium plaque predicts 5 year event probabilities in adults regardless of cholesterol results.
- Treatment with statins and other methods for lowering identified persons significantly reduces heart attack and all cause mortality.
- The cash price of testing is approximately $150.
- The test takes 10 minutes.
- The radiation exposure is minimal.
The authors conclusion: While CT scores don't identify soft plaque that can rupture and result in events, the presence of plaque in adults results in an actionable preventive recommendation that has clearly resulted in lowering events.. As part of prevention of chronic disease in our aging population, there is strong rationale for routine calcium scanning starting at age 45 years.
I would add that in my experience and backed by patient population studies, advanced lipid testing can identify persons with soft plaque at risk for rupture. Soft plaque precedes the development of calcified coronary plaque.
Dr, Kordonowy's cardiovascular disease prevention take home message:
1. Get Advanced Cholesterol Blood testing if you have a family history of heart attacks before age 65 years.
2. Persons aged 45-50 should consider a CT coronary calcium score.
In patients with family histories of early heart attacks in parents or siblings, advanced lipid testing, including checking Lp(a) and inflammatory markers, is warranted. The goal is to identify persons who are likely to follow their genetically linked associations. Additionally for the "rest" of the population
acknowledging the highest mortality besides trauma, comes from cardiovascular disease, it is suggested to get a CT calcium study as a baseline starting at age 45-50 years of age.
|
|
| Hospital Setting is Not Natural |
Spoiler alert: There is no blood pressure number that ever warrants emergency attention.
Caveat: Abnormally high blood pressure in the presence of acute delirium, neurologic stroke, acute pulmonary edema, subarachnoid hemorrhage or active angina are medical emergencies.
We often do things in the hospital that aren't necessary.
Patients, nurses and doctors have been conditioned to overreact to high blood pressure measurements. Supporting my statement is this recent article from the American Journal Of Medicine. This is an
evidence-based review of elevated blood pressure for hospitalized/inpatients. We know that sustained (years) of high blood pressure causes strokes. This is clearly true but
what is lost in translation is the myth that elevated blood pressures in the hospital setting is associated with acute strokes and death. I felt this article is especially necessary to share with patients as this objective review of the literature totally supports my 27 years of clinical experience. Following my inpatients I can vouch that our hospitals have standard hospital orders to administer a sundry of IV and oral drug remedies to treat inconveniently elevated blood pressures. The protocols are treating measurements with no documented benefits.
The opposite is true- treating blood pressure elevation with medication infusions for non emergency hypertension leads to complications including stroke.
This comprehensive review of the documented literature leads to the following clinical significance bullet points:
- Elevated blood pressure is common in patients who are hospitalized
- There are no set standards for recording blood pressure in the inpatient and numerous factors can impact the reported results (like sleep deprivation, pain, anxiety).
- There is no data that non symptom related elevated blood pressure leads to end organ damage or hypertensive emergency.
- Available literature suggests possible harm and little to no benefit in treating elevated blood pressures in the absence of symptoms (see Caveat section at top of this article).
The final take home message: Don't present yourself to a hospital, clinic or emergency room over a blood pressure measurement. It turns out seeking emergency intervention may be harmful to your health. Further, consider getting a copy of the referenced article to show your care team in the event you are hospitalized and the providers prescribe new blood pressure medications.
I will be bringing this article to the hospital medical staff for community review and discussion.
Update on Annual Screening Mammography and Breast Cancer in Women Older Than 70 Years
|
|
| Mammogram Breast Screening |
In the
February 2020 issue of the Annals of Internal Medicine the following was investigated: Estimate the effect of breast cancer screening on breast cancer mortality in Medicare beneficiaries aged 70-84 years of age. Performed was a comparison of data from 2 scenarios - annual mammograms and stopping screening. This means that symptomatic breast cases would be evaluated as is customary regardless of which arm of screening was followed.
- over a million subjects were analyzed.
- they measured 8 year breast cancer mortality, incidence of cancer and treatments plus the positive predictive value of screening.
- for women age 70-74 there were 2.7 breast cancer deaths per 1000 women who had ongoing screening versus 3.7 deaths in the "stop screening" group for a difference of one less cancer death per 1000 women screened with mammograms.
- in the age 75-80 age group there were 3.8 deaths per 1000 women who continued annual mammogram versus 3.7 deaths per 1000 women who "stopped screening".
Take home messages are among women who have at least one screening mammogram, continuing screening past age 75 year results in no material difference in cancer-specific mortality over an ensuing 8 years of follow-up. Additionally, the incidence of breast cancer and its associated mortality does increase with age. Finally, other competing reasons for death mitigate the benefit of breast screening past the age of 75 years in women.
|