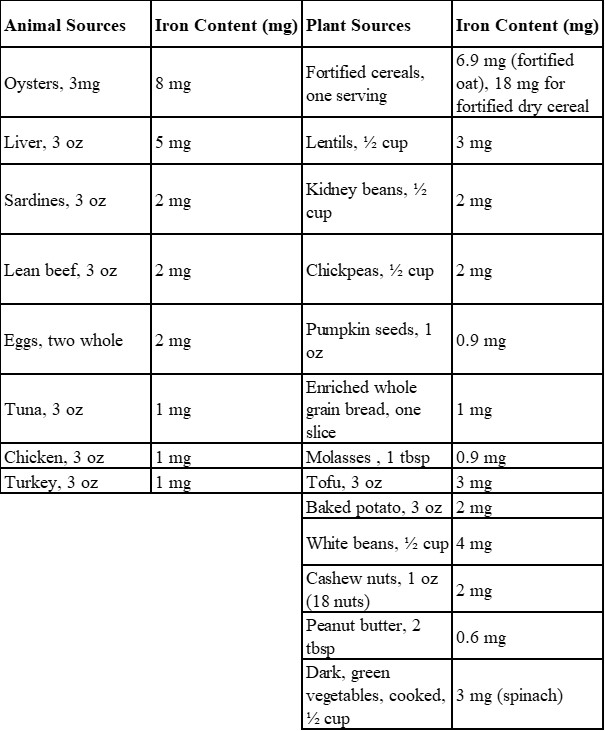
You may (or may not) have heard this before; but it is true that heme iron is better absorbed by our body. Due to this fact, many believe, (and may even have been told), that you must eat more animal products to achieve optimal iron status. Although avoiding meat can, in theory, increase your chances of iron deficiency anemia, you can sustain proper iron levels through the non-heme plant-based food sources mentioned above without incorporating beef or other red meat sources in your diet. Whether you choose to eat meat or not, you’ll want to be sure to include plenty of iron rich foods in your life each day and week. One important note: in order to improve your body's absorption of non-heme iron, pair these iron-rich plant foods with foods rich in vitamin C (citrus fruits, guava, kiwi, bell peppers, broccoli, tomatoes). Vitamin C is critical here as it acts as a reducing agent to facilitate absorption of iron from the gastrointestinal (GI) tract and allow for mobilization from storage.
Here is an easy to make, and even easier to modify, dish that can boost iron intake and status by combining non-heme iron foods with vitamin C rich foods.
Iron “Power Bowl”
Ingredients:
- Cooked beans or lentils of choice
- Diced fresh tomatoes
- Raw baby spinach
- Pumpkin seeds or cashews (nut/seed of choice)
- Raisins or dried apricots (dried fruit of choice)
*Feel free to mix and match amounts and varieties within each category above
Simple Lemon Vinaigrette
Ingredients:
- 2 tbsp lemon juice
- ½ teaspoon dijon mustard
- 3 tbsp olive oil
- 1 tbsp honey
*Feel free to start with these quantities or scale this recipe up and refrigerate any reminder for future use
Directions:
In a large bowl, combine cooked beans or lentils with diced fresh tomatoes, raw baby spinach, pumpkin seeds or cashews, and raisins or dried chopped apricots. Drizzle with the simple lemon vinaigrette above or any vinaigrette of your choice! Stir ingredients well and allow to sit for at least 15 minutes to incorporate the flavors!
Who’s At Highest Risk for Iron Deficiency?
While iron deficiency can affect all people, menstruating individuals, children, the elderly, endurance athletes, pregnant women, and people with chronic kidney failure or dialysis are at higher risk.
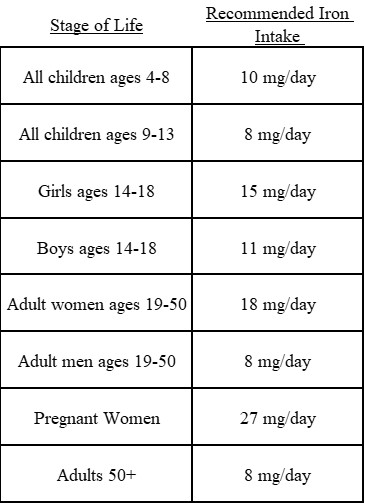
As mentioned above, The Recommended Dietary Allowance (RDA) for iron is 27 mg /day for pregnant women. Iron needs to jump up drastically during pregnancy as both the number of blood cells and blood volume increase significantly at this time. Iron is usually in prenatal vitamins given to women throughout pregnancy to meet this need and prevent complications of low iron, such as premature birth or low birth weight. As you might expect, menstruating individuals who experience heavy monthly bleeding are at a greater risk of developing iron deficiency. If this may be the case for you, refer to the iron-rich food chart attached for some ideas of ways to incorporate more good dietary iron sources into your diet, and remember to get your iron panel tested more often.
Additionally, athletes need to be particularly aware of their increased iron needs as high intensity and endurance-type exercise increases iron losses by up to 70 percent compared to sedentary populations. Athletes also lose iron through heavy sweating and increased blood loss in the urine and gastrointestinal (GI) tract. As if that weren't enough, running and other intensive training can lead to a condition known as foot-strike hemolysis, or “runner's anemia”. Foot-strike hemolysis occurs when red blood cells break down as they pass through the feet during repetitive pounding when running.
Lab Testing for Iron Deficiency Anemia
Typically, doctors will screen for anemia by checking complete blood count (CBC), including hemoglobin, hematocrit, and other factors that measure red blood cell volume and size.
Additionally, measuring levels of ferritin and transferrin can be very beneficial. Transferrin is a protein in the blood that binds to iron, regulates absorption, and facilitates the transport of iron to various tissues throughout the body. As the supply of iron in the body decreases, demand for transferrin increases, causing the lab value to increase. On the other hand, iron deficiency can be diagnosed based on serum levels of ferritin, a marker of iron storage in the liver, spleen, muscle tissue, and bone marrow. The cutoff for the first stage, mild iron deficiency, is <35 µg/L ferritin, the second stage, marginal deficiency, <20 µ/ L, and in the third stage, iron deficiency anemia, <12 µ g/ L.
Linking an athletes' ferritin level directly to their performance can be difficult because each athletes' physiology and training demands differ, making their ferritin goals vary. Even when an athletes' ferritin level is within a generally considered normal range (between 12 to 50 µ/ L), this still can indicate the development of iron deficiency and a need to intervene. Many athletes find they will perform best when their ferritin is at least 30µ/ L or ideally closer to 50 µ/ L, but it is important to speak with your doctor as well as a sports dietitian to create a plan of action for your personal needs.
Finally, total Iron-Binding Capacity (TIBC) is another useful lab to measure, since TIBC measures the blood's ability to attach itself to iron and transport it around the body. TIBC increases as iron becomes deficient.
We recommend all athletes have these tests done at least once a year, while those at higher risk of anemia would benefit from iron panel testing 2-3 times/ year; likely at the beginning of their season, prior to peak competition, and again at the end of their sports season.
Iron Interference
Staples in your diet, such as caffeine and dairy/milk can interfere with iron absorption.
But don't worry...you can still get your caffeine fix in!
Drinking coffee an hour before a meal will have almost no influence on iron absorption while drinking caffeinated beverages with iron-containing foods is associated with a 39 to 90 percent reduction in iron absorption. Even non-caffeinated coffee and tea products contain various polyphenols that have an affinity for iron when consumed simultaneously. This binding between polyphenols and iron impacts non-heme iron sources and does not affect heme iron sources.
Supplements
Iron supplements can be helpful to persons who struggle to incorporate enough iron through dietary measures alone and/or have high iron needs. When treating iron deficiency, we often start with a recommendation of 20 mg/day of elemental iron, but may go up from there depending on lab values and other factors.
When looking for an iron supplement, it is critical to note the type of iron the supplement contains. Some types of iron are absorbed more easily than others; brands such as Slow Fe Iron Tablets, Floridix Liquid Iron + Herbs and Pure Encapsulations Iron-C are absorbed well and ones we recommended often.
We also need to be aware that a high intake of fiber rich foods (bran, legumes, raw vegetables), interferes with iron absorption. This is yet another example of more is not always better. While some fiber is great for our health, there is such a thing as too much of a good thing when it comes to nutrient interactions. If you have any questions on this, please reach out to us to speak with a dietitian for more information.
Rare But True: Iron Overload
Excessive iron intake can lead to iron overload in susceptible individuals. Iron overload is a condition categorized by increased oxidative damage, polycythemia, increased blood viscosity, and increased risk of cardiovascular problems, especially when compounded by extreme heat. Iron overload is not a concern to iron-deficient individuals, but is a risk to the ~10% of the US population with hemochromatosis, who carry the gene that causes them to absorb more iron naturally. For reference, most people absorb about 10 percent of iron that they consume, whereas people with hemochromatosis absorb 30 percent, allowing the iron in their body to build up to dangerous levels.
We hope this newsletter raised your awareness and provided you with all that you needed and more to help to prevent or treat iron deficiency anemia. Speak to your dietician if you have any further questions-as always, we’d be happy to help.