1) Age: Less than one month or greater than one month?
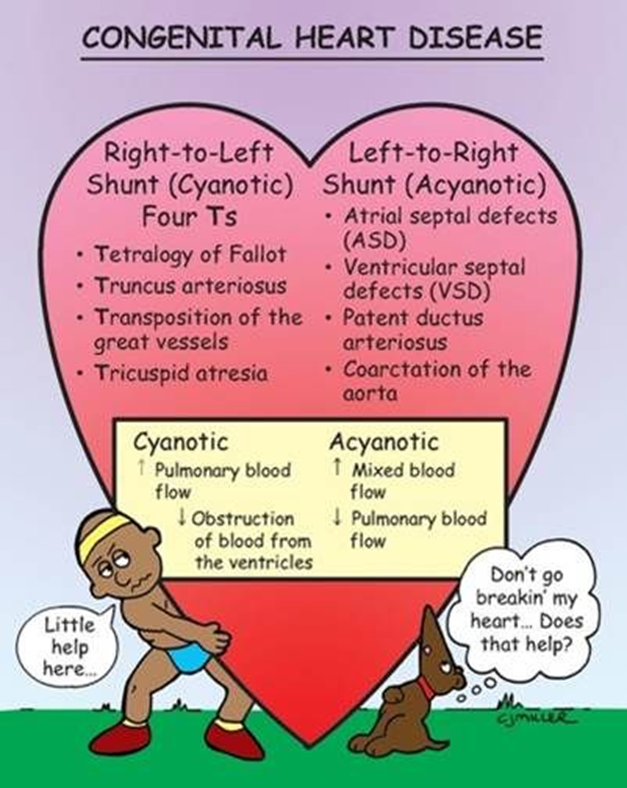
Any infant < 1 month of age with cyanosis or shock should be considered to have duct-dependent critical congenital cardiac disease until proven otherwise. This is almost always a left heart lesion/ductal dependent lesion such as Tetralogy of Fallot, which usually benefits from prostaglandins. Shunting or mixing lesions such as VSD or PDA and heart failure typically present later during infancy, usually after 1-6 months of age.
2) Color: Pink, Gray or Blue?
Pink
: think
heart failure
(adequate pulmonary blood flow, relatively well-perfused and oxygenated; usually due to a shunting lesion)
Gray
: think
shock/circulatory collapse
(not enough systemic flow, not oxygenating well; usually left-sided obstructive, ductal-dependent lesion). These patients are very sick with hypotension, tachypena and poor capillary refill. They will almost always benefit from fluids and prostaglandins if less than 1 month in age.
Blue:
think
right obstructive
duct-dependent in the first month of life
or mixing lesion
(inadequate pulmonary blood flow: usually right-sided obstructive ductal-dependent lesion or a mixing lesion) after one month of life. These patients also almost always require prostaglandins.
*
Infants struggling to breath (retractions, grunting, etc.) usually have an underlying respiratory disorder versus the infant who is displaying ‘silent tachypnea’, without increased work of breathing secondary to metabolic acidosis from a cardiac or metabolic cause.
*
To distinguish
central
cyanosis from
peripheral
cyanosis, look for bluish discoloration
inside
the mouth – tongue, mucous membranes and lips.
*Ask about timing of symptoms: Symptoms of respiratory conditions tend to start at birth as opposed to cardiac conditions that tend to present a few days after birth, when the ductus begins closing.
3) Bedside and Physical Examination Tests in Congenital Heart Disease Emergencies
Hyperoxia Test: Differentiating pulmonary disorders from cardiac disorders
The hyperoxia test was originally described using the PAO2 from the arterial blood gas. A simpler method involves using a pulse oximeter before and after the patient receives 100% oxygen for 5-10 minutes and noting whether or not the oxygen saturation improves. If the oxygen saturation improves then the underlying cause of the oxygen desaturation favors a respiratory etiology, whereas if the oxygen saturation does not improve, a cardiac cause is more likely.
Caution!
100% oxygen is a pulmonary vasodilator and could worsen respiratory distress in a patient with ductal-dependent lesions.
Pulse Delay or Absence
: Decreased or absent
femoral pulses
may suggest coarctation of the aorta
Blood pressure differential
: A difference between preductal (i.e. right arm) blood pressure and lower extremity blood pressure of > 10 mmHg, may indicate an obstructive process to the lower extremities.
ECG in Congenital Heart Disease Emergencies
Look for LVH and Persistent RVH after 1 month of age
One of the most important considerations in the infant ECG to help determine a congenital heart defect (in particular a ductal dependent lesion), is to determine whether LVH is present (abnormal regardless of age) and to determine if RVH is present after the age of one month. Normal newborns have high right sided pressures (right axis deviation) with ECG signs of RVH. High right sided pressures and RVH after one month of life is likely due to a cardiac obstructive lesion.