Florida EMSC Program Manager
Welcome new Florida EMSC Program Manager, Lorrianna Jean-Jacques! Lori previously worked with the Department of Health, Division of Emergency Preparedness and Community Support, Bureau of Public Health Pharmacy. She has worked with EMS providers through the Helping Emergency Responders Obtain Support (HEROES) Program and is a Certified Nursing Assistant.
Florida EMSC Advisory Committee Meeting
Join us for our quarterly meeting on Wednesday, October 23 at 1:00 pm at World Golf Village Renaissance in St. Augustine, FL, room: St. Augustine FG.
|
|
Encourage others to sign up for the PEDReady weekly newsbrief, the PE
2
ARL, by sharing this link:
http://bit.ly/flpearl
|
|
Focus |
Importance of Communication in Pediatric Emergency Care to Improve Patient Safety & Reduce Malpractice Claims
|
|
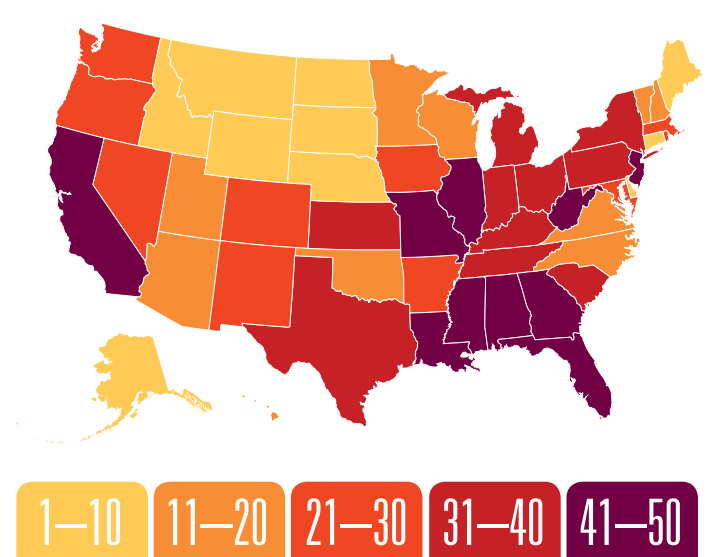
Did you know that a
2019 survey
ranks Florida’s lawsuit climate among the nation’s worst in multiple categories?
|
|
There are limited studies regarding
pediatric specific
malpractice claims, especially for the emergency department (ED). Yet a recent
study of malpractice claims involving children
highlights the role of communication and system issues as contributing factors to lawsuits.
This 10-year study is important because it focuses exclusively on children and provides data on the top specialties named as defendants, including emergency medicine. The study includes real-life case examples that demonstrate problems are not usually caused by physician/nurse lack of knowledge. Instead, most errors are caused when things fall through the cracks due to system issues, including communication.
The study found communication breakdowns between patients/families and providers contributed to 15-22% of claims
.
Communication gaps are particularly risky when treating young children. Consider that when dealing with pediatric cases, you have a minimum of two patients: the child and parent or guardian, plus the actual current caregiver, grandparents, coaches, teachers, siblings, etc. System issues often contribute to communication failures, such as when a child’s previous electronic medical records cannot be found because of a misspelled name from the field or when using an incorrect date of birth.
This study also draws attention to errors that are related to test results. For example, lost results, failure to inform physicians of critical test results, or not understanding normal pediatric lab value variation by age.
Click here
to review a PEDReady resource containing pediatric lab values by age.
Having a clear call-back system and policies for reviewing diagnostic test results is key to preventing these system errors. It is important to always confirm the best phone number whereby ED staff can reach the parent to report abnormal results or arrange follow-up.
|
|
How can we make children, parents & emergency providers better partners in our medical process and decrease our liability and exposure to malpractice claims?
|
|
The ED and EMS settings are particularly high-risk because of critical conditions, rushed conversations, teams assembled ad hoc, and lack of prior patient knowledge or relationship. We have to become experts at putting children and their anxious parents at ease in seconds, while obtaining critical information from someone we have never met and complete a brief assessment—all at the same time! That is what makes you a PEDReady Champion.
|
|
Be cognizant of these pediatric high-risk scenarios:
|
|
- Newborns and neonates
- Children returning to ED or doctor’s office for > 2 visits or repeat EMS calls
- Children with special health care needs or technology dependent children
- Tracheostomies, feeding tubes, VP shunts, etc.
- Children returning with post-surgical complaints
- Children/parents with limited English proficiency, disabilities, chronic or mental conditions
- Unimmunized children
- Abnormal vital signs
- High-risk chief complaints such as testicular pain, respiratory distress, seizures or fever
- Beware of “it’s just a febrile seizure”
|
|
Have a communication plan or protocol and use the ABCs (Always Be Consistent)
|
|
-Always identify your role, who is with the child and their role
- Consistently start by saying, “hello I am Dr. X (or nurse, paramedic, etc.) and this is? (point/motion toward child/baby and wait for response of child’s name)? And you are? (if appropriate, shake hands or touch arm and determine caregiver/adult’s name and relation to your patient)."
- Just remember: "I am…, this is….? you are…?" Obviously this approach will need to be adjusted in critical scenarios.
|
|
Thanks to Dr. Peter Antevy for sharing his approach to this issue!
|
|
- Don’t assume the accompanying adult at the scene or in the ED is the parent or legal guardian
- Determine who actually cares for the child on a regular basis; who witnessed the accident, event, etc.?
- Double check spelling of name and DOB as correcting this later is difficult and leads to missed opportunities in reviewing existing medical records or immunization registries
- Beware of templated EMR checkboxes; always add a few details like “patient smiling, playful and grabbing stethoscope”
- If encountering non-English speaking patients/caregivers, try using Florida PEDReady communication cards or a phone app until an interpreter system is available
- Click here to download a copy or email pedready@jax.ufl.edu
“The most important thing in communication is hearing what isn’t said" —
Peter Drucker
|
|
 |
The following is a condensed version of "
When Treating Kids, Learn from the ED,"
published in
EMpulse Fall 2019
.
Click here
for the full article as a PDF.
|
|
|
|
Four Pediatric Communication Lessons Learned from the ED:
|
|
1. Understand Discharge Instructions
|
|
Case example:
A mother brought her 10-year-old son to the ED with abdominal pain. Following examination and testing, he was discharged home after verbal and written instructions to return immediately for worsening or red-flag symptoms.
Over the next 48 hours, the child did display worsening symptoms.The mother scheduled an office appointment for the next day. After the boy began vomiting blood, 911 was called and paramedics transported him to the ED in cardiac arrest. He died as a result of a perforated appendix.
Lesson:
Both verbal and written discharge instructions are important, and must be presented in layperson’s terms. Printed EHR instructions are complex and lengthy; highlight key features and phone numbers. Three key components include: Follow-up details, disease red flags, and patient/family understanding of treatment plan (antibiotics, antipyretics, or subspecialty referral). Indicate when the patient should return for follow-up, whom to call, level of urgency, and location.
Try to determine if the child has an existing relationship with a primary care physician (PCP) or subspecialist(s). Make sure the caregiver knows the name of the child’s plan, designated PCP, and contact information.
|
|
2. Avoid Vaccination History Assumptions
|
|
Case example:
An eight-month-old infant presented to the ED during peak bronchiolitis season with a fever of 102.8°F. The parent gave a history of all shots being up to date. The patient was discharged with a diagnosis of upper respiratory infection and bronchiolitis but returned two days later with pneumonia and sepsis. On further inquiry, the parent was not the regular caregiver and the immunizations were not current.
Lesson:
When treating children under two years, always take a detailed history regarding immunizations, neonatal history, and risk factors such as prematurity. Parents often incorrectly indicate immunizations are up to date. Check immunization status by asking to review the child’s immunization card and review the EHR and state immunization registry. Febrile children without current immunizations may require additional evaluation, and are at greater risk for serious bacterial disease. This is especially true for those under six months of age.
|
|
Case example:
Paramedics transported an African American teenager with pain and gave an ED triage report that the young man had sickle-cell disease, had not attempted any pain relief medications, and was possibly a drug seeker. This same information was related to the ED physician, who initially approached the patient with frustration, but took time to ask additional questions, including some ice-breaker questions: “Where do you go to school?” and “Tell me what you know about your disease.” The physician discovered the patient was an honors student at a prestigious university. He did not have sickle cell but another hematologic condition. He was visiting grandparents and his pain medications were in his out-of-town dorm room.
Lesson:
Always confirm key elements of the history. It is difficult to get a correct history in a brief encounter, especially with someone you are meeting for the first time. Ask patients and/or parents some nonmedical
getting-to-know-you
questions, and confirm the relationship of adults accompanying the child, the primary caregiver, and the child’s level of functioning. What grade are they in? Has their activity level changed? Speak directly to the child and allow the child to tell part of their story.
|
|
4. Ask the Right Questions
|
|
Case example:
A mother presented her child to ED registration with a chief complaint of fever. The child had no fever and was playful. In fact, the mother was concerned her child had been abused while staying with the father over the weekend. The mother did not wish to report this concern at check in, and stated she was scared of her child’s father.
Lesson:
Do read triage and staff notes, but begin your conversation with the open-ended question: “What are you most worried about today?” This may reveal the true most pressing concern.
Finally, rapport matters. No matter how strong your emotional intelligence, you can’t communicate well with everyone. A patient may be willing to confide in a female physician but not a male or understand one physician’s way of explaining things better than another’s. If you are not having successful communication, consider including another provider or staff member in the conversation.
|
|
PEDReady Champions of the Week:
|
|
Walton County Fire Rescue
Congrats to Sarah Earley and her team for their efforts to be
PEDReady!
Sarah is the Field Training Evaluation Program Coordinator for Walton County Fire Rescue and the newest Florida PECC (Pediatric Emergency Care Coordinator/Champion). Take a look at these awesome photos with Walton Co. Fire Rescue showing off their PEDReady Toolkit materials!
|
|
Upcoming Pediatric Emergency Events
|
|
2019 Bay Area Trauma Symposium
October 29-30, 2019 | St. Petersburg, FL
Hosted by: Bayfront Health St. Petersburg & Johns Hopkins All Children's Hospital
Experts in pediatric and adult trauma will discuss a range of current issues. Day 1 will cover pediatric trauma; day 2 will cover adult trauma. Registration fee is $25/day.
|
|
|
Webinar: Using Fatality Review to Understand Disasters
(new)
October 31, 2019 at 2:00 pm
Hosted by: EMSC IIC
This webinar will focus on common definitions of a disaster, best practices in fatality reviews when a disaster occurs, and available resources for children. Examples of how CDR and FIMR teams have used fatality review to gain a deeper understanding of disaster events will be shared.
Changes to the National Fatality Review-Case Reporting System will also be discussed.
|
|
|
NAEMT Principles of Ethics & Personal Leadership Course
November 6-7, 2019 | 8:30-4:30 pm | St. Augustine, FL
Hosted by: TraumaOne Flight Services
This 2-day (16-hour) course provides EMS and Mobile Healthcare (MHC) practitioners with the skills to effectively interact with patients and their families, other medical personnel, co-workers, supervisors and community residents. This course is appropriate for EMTs, paramedics, other MHC practitioners and emergency responders. Upon successful completion, students receive a certificate, wallet card
(good for 4 years) and 16 hours of CAPCE credit.
|
|
|
Pediatric Care After Resuscitation (PCAR) Course
Dec 2-3, 2019 | Jacksonville, FL
The mission of TCAR (Trauma Care After Resuscitation) Education Programs is to expand the knowledge base and clinical reasoning skills of nurses who work with injured patients anywhere along the trauma continuum of care, particularly in the post-resuscitation phase.
|
|
|
Thanks for being a Pediatric Champion!
|
|
The Florida PEDReady Program
|
|
|
|
|
|
|
|