|
|

|
|
I hope this newsletter finds you and your family well. It's hard to believe that the holiday season is in full swing. I hope everyone gets to enjoy time with family and friends. I was at the Iron Bowl game last weekend (Alabama vs Auburn). What a great environment! The place was full of crazy passionate fans, just what college football should be. Although the outcome wasn't what I hoped (my daughter goes to Alabama) we had a great time. Hopefully, now the Badgers can win their way into the playoff!
The first article is nuts. As in, nuts are good for you, really good for you. Not many things can get you a 15-23% reduction in heart disease. Read on to get the specifics of how much and what type I recommend.
I am always looking at way to assess risk. I don't want to under treat, but also don't want to over treat my patients. Looking for painless, cost-effective tests that can give good information is something I'm always open to. The second study describes one of these tests. It's cheap, easy, painless and the information can be extremely beneficial.
Eczema is a skin disorder that affects many of us, especially in the winter when the air is cold and dry. Our skin is dry, cracking and itchy. Many of us have tried various creams and lotions. The third article shows us that good "bugs" may be helpful in avoiding the issues that go along with eczema.
Click on the links the the left to check out our redesigned
web site
...
|
|
That's Nuts!
|
Nut consumption reduces cardiovascular disease
This study published in the
Journal of the American College of Cardiology evaluated nut consumption and rate of cardiovascular disease in over 210,000 subjects over 5 million person-years of follow up and found that those who ate a handful of nuts 5 days/week had significantly reduced total cardiovascular disease and coronary heart disease.
Abstract:
- Background The associations between specific types of nuts, specifically peanuts and walnuts, and cardiovascular disease remain unclear.
- Objectives The authors sought to analyze the associations between the intake of total and specific types of nuts and cardiovascular disease, coronary heart disease, and stroke risk.
- Methods The authors included 76,364 women from the Nurses' Health Study (1980 to 2012), 92,946 women from the Nurses' Health Study II (1991 to 2013), and 41,526 men from the Health Professionals Follow-Up Study (1986 to 2012) who were free of cancer, heart disease, and stroke at baseline. Nut consumption was assessed using food frequency questionnaires at baseline and was updated every 4 years.
- Results During 5,063,439 person-years of follow-up, the authors documented 14,136 incident cardiovascular disease cases, including 8,390 coronary heart disease cases and 5,910 stroke cases. Total nut consumption was inversely associated with total cardiovascular disease and coronary heart disease after adjustment for cardiovascular risk factors. The pooled multivariable hazard ratios for cardiovascular disease and coronary heart disease among participants who consumed 1 serving of nuts (28 g) 5 or more times per week, compared with the reference category (never or almost never), were 0.86 (95% confidence interval: 0.79 to 0.93; p for trend = 0.0002) and 0.80 (95% confidence interval: 0.72 to 0.89; p for trend <0.001), respectively. Consumption of peanuts and tree nuts (2 or more times/week) and walnuts (1 or more times/week) was associated with a 13% to 19% lower risk of total cardiovascular disease and 15% to 23% lower risk of coronary heart disease.
- Conclusions In 3 large prospective cohort studies, higher consumption of total and specific types of nuts was inversely associated with total cardiovascular disease and coronary heart disease.
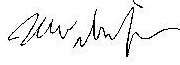
This very large and prolonged study proves that consumption of nuts is beneficial. Those consuming around 1 oz of nuts 5 or more days weekly had a 13-19% lowered risk of total cardiovascular disease and 15-23% lower risk of coronary heart disease. That is a significant decrease and shows that nuts, high in fiber and healthy omega-3 fats should be a part of our diets. This study did include peanuts, which are actually legumes and I would recommend sticking with the tree nuts for the most part. These can be included as a nice snack or as part of a salad or other dish. I would remove them from the can or bag as it is easy to consume a lot more than an ounce at one sitting. I also recommend raw over roasted whenever possible as this may convey some other benefits outside of less cardiovascular disease. Enjoy!
- Almonds (20 - 24 nuts): 160 calories, 14 grams fat, 6 grams protein
- Brazil Nuts (6 - 8 nuts): 190 calories, 19 grams fat, 4 grams protein
- Cashews (16 - 18 nuts): 160 calories, 14 grams fat, 4 grams protein
- Hazelnuts (18 - 20 nuts): 180 calories, 17 grams fat, 4 grams protein
- Macadamia (10 - 12 nuts): 200 calories, 22 grams fat, 2 grams protein
- Peanuts (28 nuts): 170 calories, 14 grams fat, 7 grams protein
- Pecans (18 - 20 halves): 200 calories, 20 grams fat, 3 grams protein
- Pine Nuts (150 - 157 nuts): 160 calories, 14 grams fat, 7 grams protein
- Pistachios (45 - 47 nuts): 160 calories, 13 grams fat, 6 grams protein
- Walnuts (14 halves): 190 calories, 18 grams fat, 4 grams protein
|
A Better Test For Prognosis
|
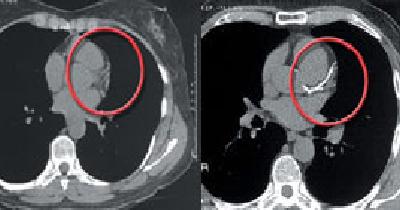
Heart scan helps to better assess risk of CV disease
I am always looking at ways to assess risk in my patients to prevent disease. But I also want to be sure that I am not over treating and giving medications unnecessarily. This study, published in JAMA Cardiology shows that coronary artery calcium scans (heart scans) added both prognostic value to assessment of heart disease and could also able to help avoid over treatment of risk factors.
Abstract:
- Importance: Although the risk of type 2 diabetes is considered to be equivalent to coronary heart disease (CHD) risk, there is considerable heterogeneity among individuals for CHD and atherosclerotic cardiovascular disease (ASCVD) risk. It is not known whether coronary artery calcium (CAC) assessment at baseline in individuals with established metabolic syndrome (MetS) or diabetes identifies CHD and ASCVD prognostic indicators during a long follow-up period.
- Objective: To compare improvement in long-term prognostication of incident CHD and ASCVD using CAC scores among those with diabetes, MetS, or neither condition.
- Design, Setting, and Participants: This study included participants from the Multi-Ethnic Study of Atherosclerosis (MESA), a prospective cohort study of 6814 males and females aged 45 to 84 years without known CVD from 4 race/ethnicity groups (white [38.5%], African American [27.5%], Hispanic [22.1%], and Chinese [11.9%]) recruited from 6 US communities from July 2000 through August 2002. Follow-up for each participant extended to the first occurrence of an incident event, other death, loss to follow-up, or the last follow-up call through December 31, 2013. Data analysis was performed from June 1, 2016, to September 12, 2017. Cox proportional hazards regression models were used to estimate hazard ratios (HRs). Area under the receiver operator characteristic curve and net reclassification improvement were used to compare incremental contributions of CAC score when added to the Framingham risk score, ethnicity/race, and socioeconomic status.
- Main Outcomes and Measures: CHD events, including myocardial infarction, resuscitated cardiac arrest, or CHD death.
- Results: Of 6814 MESA participants, 6751 had complete risk factor and follow-up data and were included in this study (mean [SD] age, 62.2 [10.2] years; 3186 [47.2%] male). A total of 881 (13.0%) had diabetes, 1738 (25.7%) had MetS, and 4132 (61.2%) had neither condition. After 11.1 mean years of follow-up, CHD events occurred in 84 participants with diabetes (135 ASCVD events), 115 with MetS (175 ASCVD events), and 157 with neither (250 ASCVD events). The CAC score was independently associated with incident CHD in multivariable analyses in those with diabetes (HR, 1.30; 95% CI, 1.19-1.43), MetS (HR, 1.30; 95% CI, 1.20-1.41), and neither condition (HR, 1.37; 95% CI, 1.27-1.47). For incident CHD, net reclassification improvement with addition of CAC score was 0.23 (95% CI, 0.10-0.37) in those with diabetes, 0.22 (95% CI, 0.09-0.35) in those with MetS, and 0.25 (95% CI, 0.15-0.35) in those with neither condition. The CAC score was also a prognostic indicator of CHD and ASCVD after controlling for diabetes duration of 10 years or longer at baseline, insulin use, and glycemic control.
- Conclusions and Relevance: In a large multiethnic cohort, the addition of CAC score to global risk assessment was associated with significantly improved risk classification in those with MetS and diabetes, even if diabetes duration was longer than a decade, suggesting a role for the CAC score in risk assessment in such patients.
Everyone is different. This seems to be common sense, but in the way we treat people medically this isn't always true. We see a diagnosis such as diabetes or metabolic syndrome and assume there is coronary artery disease. While this is often true it isn't universal. So who should be targeted for intense intervention? We need more information. This study looked at an inexpensive test, a heart scan, and found that it was very helpful in the prognosis of overall cardiac risk. I often recommend this inexpensive test ($129-$199 locally) to get more information and this study backs up my reasoning. A calcium score of 0 means low risk and no need for intervention. A high calcium score means we should do more work up, assessment of risk, and review interventions. In medicine we are always looking at ways to intervene, but this is a test that is also helpful to avoid excess intervention.
|
|
Bugs For Your Rash
|
Probiotic reduces severity of eczema and topical steroid use

Eczema,
also called dermatitis is a common skin disorder, especially in children. It is characterized by dry, itchy skin and
rashes on the face, inside the elbows and behind the knees, and on the hands and feet. It often causes scratching which can cause the skin to turn red, swell and itch even more.
The cause is not known but it is likely caused by both genetic and environmental factors.Treatment is generally with moisturizing lotions and creams along with topical steroids such as hydrocortisone or other stronger types. This study found that taking a mixture of probiotic strains reduced both the bothersome symptoms of eczema as the need for steroid creams.
Abstract:
- Importance: Oral intake of new probiotic formulations may improve the course of atopic dermatitis (AD) in a young population.
- Objective: To determine whether a mixture of oral probiotics is safe and effective in the treatment of AD symptoms and to evaluate its influence on the use of topical steroids in a young population.
- Design, Setting, and Participants: A 12-week randomized, double-blind, placebo-controlled intervention trial, from March to June 2016, at the outpatient hospital Centro Dermatológico Estético de Alicante, Alicante, Spain. Observers were blinded to patient groupings. Participants were children aged 4 to 17 years with moderate atopic dermatitis. The groups were stratified and block randomized according to sex, age, and age of onset. Patients were ineligible if they had used systemic immunosuppressive drugs in the previous 3 months or antibiotics in the previous 2 weeks or had a concomitant diagnosis of intestinal bowel disease or signs of bacterial infection.
- Interventions: Twelve weeks with a daily capsule containing freeze-dried powder with 109 total colony-forming units of the probiotic strains Bifidobacterium lactis CECT 8145, B longum CECT 7347, and Lactobacillus casei CECT 9104 and maltodextrin as a carrier, or placebo (maltodextrin-only capsules).
- Main Outcomes and Measures: SCORAD index score and days of topical steroid use were analyzed.
- Results: Fifty children (26 [50%] female; mean [SD] age, 9.2 [3.7] years) participated. After 12 weeks of follow-up, the mean reduction in the SCORAD index in the probiotic group was 19.2 points greater than in the control group (mean difference, -19.2; 95% CI, -15.0 to -23.4). In relative terms, we observed a change of -83% (95% CI, -95% to -70%) in the probiotic group and -24% (95% CI, -36% to -11%) in the placebo group (P < 0.001). We found a significant reduction in the use of topical steroids to treat flares in the probiotic arm (161 of 2084 patient-days [7.7%]) compared with the control arm (220 of 2032 patient-days [10.8%]; odds ratio, 0.63; 95% CI, 0.51 to 0.78).
- Conclusions and Relevance: The mixture of probiotics was effective in reducing SCORAD index and reducing the use of topical steroids in patients with moderate AD.
Eczema is very common in children and adults. It causes itching, rashes and general discomfort. We often prescribe steroid creams and ointments to treat this but longer term use of these products can have side-effects. This study shows that a safe, cheap intervention can be beneficial for kids (and likely adults) who have skin issues due to eczema. There have been multiple studies over the years showing benefit. Studies have even shown a benefit when given to pregnant women who have eczema with less eczema in her child. I recommend a probiotic with multiple species and around 20 billion colonies/capsule. I carry a good brand at my office or probiotics are available at most health food stores and pharmacies.
|
|
Thank you for taking the time to read through this newsletter. I hope you have found this information useful as we work together to optimize your health.
As always, if you have questions about anything in this newsletter or have topics you would like me to address, please feel free to contact me by
email
, phone, or just stop by!
To Your Good Health,
Mark Niedfeldt, M.D.
|
|
|