|
|
MUSC Otolaryngology - Head & Neck Surgery E-Update May 2017
|
|
Greetings Colleagues!
Our ENT E-Updates are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. I hope you are finding these newsletters useful. Your feedback or questions about the E-Update articles, your patients, or any other ENT issue are always welcome. Write to us at [email protected] - And please forward this E-Update to your colleagues who may also benefit from sharing the latest ENT topics. As always, your support is deeply appreciated.
Yours sincerely,
Paul R. Lambert, M.D.
Professor and Department Chair
|
Empty Nose Syndrome: Renewed Interest in Diagnosis and Treatment Outcomes
Zachary M. Soler, M.D., MSc
|
Empty nose syndrome (ENS) has always been a controversial disease entity. Some have argued that it is primarily a psychologic problem manifesting itself in nasal symptomatology. Others have argued that psychologic issues are a downstream consequence and that its true pathophysiology relates to abnormal nasal airflow. Regardless, the general sentiment was that little could be done to ease their symptoms and that patients who suffered with this condition were difficult to manage and best avoided. However, there has been renewed interest in ENS over the last few years, with research focusing on diagnostic accuracy, surgical treatments, and improved analysis of outcomes.
Patients with ENS classically complain of difficulty breathing through their nose, often feeling that not enough air moves their nose and that they have an almost suffocating feeling. Sometimes this is accompanied by dryness, crusting, and burning. The vast majority of patients have had prior nasal surgery, often with significant turbinate reductions. Paradoxically, when one looks into the nose, the nasal cavity is typically wide open and thus the volume of air moving with inspiration is quite large. What is perplexing to many physicians is that these symptoms are not experienced uniformly across all patients who have had aggressive nasal mucosal resection. Two separate patients may have identically-appearing nasal cavities on endoscopy yet one is debilitated by symptoms and the other feels great.
|
Figure 1. Coronal computed tomography (CT) scan of patient with empty nose syndrome showing inferior and middle turbinate resections, along with compensatory hypertrophy of septal mucosa.
|
Proper diagnosis of ENS is critical in order to guide patient counseling and future treatment recommendations. Ideally, one would document the presence of 4 key features in order to be secure in the diagnosis: characteristic symptoms, history of prior nasal resection, endoscopic or radiographic appearance, and a positive cotton ball test. When it comes to symptoms, the exact description can vary across patients and at times be hard to discern from common entities such as chronic rhinitis. Recently, the Empty Nose Syndrome 6-Item Questionnaire (ENS6Q) was developed and validated as a tool that can be used for both diagnosis and as an outcome metric
1. This survey is easy to administer and scores >10.5 can be used as a cut-off to identify those likely to have empty nose (sensitivity=86.7%, specificity=96.6%). The vast majority of patients will have a history of nasal surgery, most commonly inferior turbinate resection or combined inferior and middle turbinate resections. There are some patients who have rhinotillexomania (habitual nose picking) as a cause of nasal tissue loss. It is important to examine the nose thoughtfully, confirming absence of tissues and evidence of compensatory hypertrophy, often of septal mucosa adjacent to the resected turbinates. Computed tomography (CT) scanning is not compulsory, but often rules out sinusitis and can show areas of resection and compensation
(Figure 1)
2. Lastly, the "cotton test" can be administered. In this test, saline-soaked cotton is used to partially block the nose, usually in the areas where tissue has been overly resected
3. When positive, patients will describe an improvement in their subjective symptoms when partially blocked by cotton.
The pathophysiology of empty nose syndrome is controversial and mainly theoretical. One thought is that the sensation of proper airflow requires the detection of air flowing over mucosal surfaces, perhaps through temperature changes
4. Therefore, absence of this mucosa would decrease the sensation of airflow, either directly or via changes in laminar flow. The absence of tissue and turbulent flow might also reduce the ability to humidify air, resulting in dryness and crusting. Lastly and perhaps most importantly, is the concept of nasal resistance. Air is pulled into the nose during inspiration by negative pressure, overcoming the intrinsic resistance of the nasal cavity. When the turbinates are absent, this resistance is reduced and may be detected by the patient and interpreted as absence of breathing and/or feelings of suffocation
5.
Treatment of empty nose syndrome requires empathy and a holistic approach that incorporates mind and body. Like most conditions, treatment begins with education. It is critical to teach the patient why they have this condition and reinforce the concept that more tissue resection is not the answer and in fact will make things worse. Those with psychologic impacts, whether it be anxiety, depression, or obsessive-compulsive tendencies should be appropriately referred and treated. In many instances it is irrelevant whether psychologic issues were predisposing or purely a downstream impact; what is important is that they are addressed prior to and concurrent with other treatments. In many instances, medications can be used to alleviate some nasal symptoms. This might include saline gel solutions or humidification of air to improve dryness and crusting. Some patients will routinely utilize a cotton plug to partially occlude the airway. Topical menthol may improve some symptoms.
|
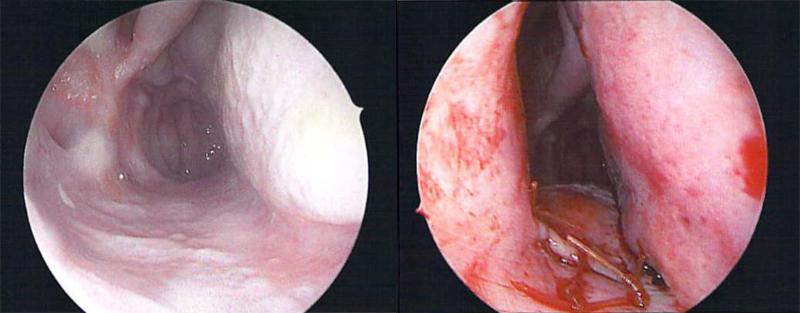
Figure 2. A) Right nasal cavity at baseline. B) Right nasal cavity after alloderm implants to bulk septum, lateral wall, and nasal floor.
|
A number of surgical procedures have been described to treat empty nose syndrome, all of which attempt to add bulk to the nasal cavity to increase surface area, alter nasal airflow, and increase nasal resistance. Reports have described injections of fillers, such as hyaluronic acid, which can bulk the residual turbinate or septum
6. These series are typically quite small and although no complications are have been reported one should remain aware that in rare instances intra-nasal injections containing particulate matter have resulted in blindness. Because injections would typically be of transient benefit, most surgeons favor more permanent procedures. These bulking procedures usually involve elevating a submucosal pocket that can be done at the location of the residual turbinate or in the inferior meatus laterally, the nasal floor inferiorly, and the septum medially. The location and size of these pockets are typically tailored to the individual patient
(Figure 2). Implant materials have included alloderm, cartilage, and porcine small intestine. A recent review systematically described published outcomes after these procedures
7. The vast majority of studies report statistically and clinically significant improvements in sinonasal QOL, including generic instruments such as the SinoNasal Outcomes Test (SNOT-20 and SNOT-25).
On a personal level, I have taken great satisfaction in caring for patients with empty nose syndrome. One only needs to peruse the patient websites dedicated to this disease or listen to the many podcasts to glimpse the disability felt by these patients and see the opportunity which exists to help8. A renewed interest among surgeons and researchers has given otolaryngologists the tools to more accurately diagnose and competently treat this condition.
|
References
- Velasquez N, Thamboo A, Habib AR, Huang Z, Nayak JK. The Empty Nose Syndrome 6-Item Questionnaire (ENS6Q): a validated 6-item questionnaire as a diagnostic aid for empty nose syndrome patients. Int Forum Allergy Rhinol. 2017;7:64-71.
- Thamboo A, Velasquez N, Ayoub N, Nayak JV. Distinguishing computed tomography findings in patients with empty nose syndrome. Int Forum Allergy Rhinol. 2016;6:1075-1082.
- House SM. Surgical treatment for empty nose syndrome. Arch Otolaryngol Head Neck Surg. 2007;133(9):858-863
- Sozansky J, Houser SM. Pathophysiology of empty nose syndrome. Laryngoscope 2015; 125:70-74.
- Swift AC, Campbell IT, McKnown TM. Oronasal obstruction, lung volumes, and arterial oxygenation. Lancet, 1988; 1 (8577):73-5.
- Modryznski M. Hyaluronic acid gel in the treatment of empty nose syndrome. Am J Rhinol Allergy 2011; 25: 103-6.
- Leong SC. The clinical efficacy of surgical interventions for empty nose syndrome: a systematic review. Laryngoscope, 2015; 125:1557-1562.
- Empty Nose Syndrome Association Web site. http://www.emptynosesyndrome.org. Accessed April 2017.
|
|
|
Zachary M. Soler, M.D., MSc
Associate Professor
Rhinology & Sinus Surgery
M.D.: Wake Forest University
Residency: Oregon Health and Science University
Fellowship: Harvard Medical School
|
|
E-Update Articles
Look for these articles in upcoming issues
June:
Resident Education in Otolaryngology
July:
Salivary Endoscopy: A Minimally Invasive Approach to Salivary Gland Disease
August:
Down syndrome and obstructive sleep apnea
To view any of our past E-Updates visit our
|
|
|
|
|
|
|
|
|