UCSF ADVANCED PRACTICE NEWSLETTER
July 2019
|
|
CELEBRATING PROFESSIONAL
NURSE PRACTITIONERS
NURSE ANESTHETISTS
PHYSICIAN ASSISTANTS
NURSE MIDWIVES
|
|
Message from Mitch Erickson, NP
Director of Advanced Practice
UCSF Health
|
Several of you may have already heard I am retiring on September 27th, 2019. I will be involved in the search committee to identify a replacement or possible interim Director. I have worked at UCSF Health for nearly 30 years and that journey has led me to all of you. You are all part of an amazing and dynamic team of advanced practice professionals. We have worked together on several fronts to both identify and recognize your contributions to this organization and our patients and support your desire to engage in the academic mission. There will always be more opportunities to improve by creating a better work environment and more importantly, a better patient experience. There are many challenging financial issues at our door that are outside our control. We will get past these challenges as long as all are mindful of our roles in meeting these challenges, small and large. Change will eternally be at our side and our success will be measured by our ability to embrace those changes. I will not be far away as I will likely engage in completing a couple projects that I will not have time for during my remaining tenure. I know you will guide my successor as you have guided me, to best represent your interests and be your voice at UCSF Health. You all have my greatest admiration.
|
|
|
IN THIS ISSUE
Highlighting AHP Practice at UCSF Health
Article by Laura Quill, PNP regarding ACE in Pediatrics
AHP UPDATES
Exceptional AHP Award Nominees and Recipients
Informed Consent Policy
Highlights of the UCSF SON DNP Program
Open Forum Highlights
NP3 Promotions
NPS Data Sharing
Inpatient Documentation Workflow and Workflow Compliance
AHP Academic Stipend
BRN Important Updates
Michelle Klosterman and Jason Wong Story
Medi-Cal SPA Time Study for Ambulatory Providers
AHP Communication Committee and UCSF AHP Chatter Instructions
New AHP AHA Re-Certification Workflow
Schwartz Rounds
Burnout in Health Care
GME Grand Rounds
New AHPs to UCSF Health for the 9th Cohort in 2019
Advisory Board Minutes - April 2019
California Healthcare News
UCSF Health Events Calendar
Center for the Enhancement of Communication in Healthcare
True North Metrics
AHP Students at UCSF Health
Sharing your Expertise across the State and Nation
Caring for the Caregiver
SON Preceptor Opportunities and UCSF Health Preceptor Training
RECOGNITION, PUBLICATIONS, AND PRESENTATIONS
Danielle Krieger, NP
Eliana Agudelo, PA
Claudia Praglin, NP
Maura, O;Day, NP
Anna Marie Torres, NP
Mitchel Erickson, NP
Marilyn McEnhill PNP
Giulia Worner NP
ONE GOOD THING
Compliments of Diane Sliwka, MD
RESOURCES
Fun Discounts for UCSF Employees
Pager Box Update
2018/2019 AHP Advisory Board
Required Training in LMS
Face Card Process
How To Correct The Staff Directory
AHP Resource Manual Link
Adding New Privileges
Scope Of Practice Details
Licensing and Certification Responsibilities
CURES Sign Up for Scheduled Medication Prescribing
BRN Link
DEA
|
|
HIGHLIGHTING THE ADVANCED HEALTH PRACTITIONERS
|
|
Article by: Laura Quill, PNP
|
|
Adverse Childhood Events (ACEs)
|
I have been a pediatric nurse and nurse practitioner for 30 years. I have spent most of my career working with children who have chronic illness (sickle cell disease). It has been increasingly visible to me that so many of the patients and families I have come to know are in need of profound healing and increasingly difficult to treat. This dyad of poorly controlled disease, poor quality of life, along with few aspects of medical care provided that hold real traction for these patients became an area of interest to me. I was able to pursue my learning on this topic with the support of the AHP education tuition fund and attended the National Adverse Childhood Event’s Conference in San Francisco this past November 2018.
What we now call Adverse Childhood Events (ACEs) a discrete group of originally 8 types of trauma that essentially fall in 3 domains; abuse, neglect, or severe family dysfunction or disruption, was originally coined in the 1980’s by Vincent Felitti, a physician and chair of the Preventative Medicine Department at Kaiser Permanente, in San Diego. He ran a trial intended to help morbidly obese patients achieve a healthy weight safely. To his surprise, he discovered that morbid obesity was linked with childhood trauma and further showed it was often physically and emotionally protective. This initial work was the groundwork for the Adverse Experiences in Childhood (ACE’s) study that he and Robert Anda from the CDC published in 1998. The ACE study screened over 17,000 adults seen at KP with a questionnaire asking about the 8 types of trauma and health. Two thirds of a primarily middle socioeconomic Caucasian sample screened positive for at least 1 ACE and eighty percent of those had two or more ACEs. The findings established a dose response to trauma and ACEs rarely occurred in isolation and increased over a patient’s lifetime. Trauma score of 4 or more was strongly linked to patients with decreased life expectancy by 20 years, chronic heart disease, stroke, high risk behaviors for drug and alcohol abuse, and mental illness. The odds ratio on developing cancer, chronic lung disease, hypertension, suicide were significant.
Despite this being a public health issue, little really moved the needle in terms of how chronic disease and mental illness were being treated over the next 2 decades. In 2008, Nadine Burke Harris a pediatrician in Bayview Hunter’s Point, SF describes seeing way too many young children sick with interruptions in normal growth, learning, and development. Rates of asthma, infection, poor growth, school failure, depression were exceedingly high. She and colleagues harnessed the profound conclusions from the ACE study and went on to screen all patients and caregivers in their practice for ACEs. Children with ACE scores of 4 or more had increased risk of disease, ADHD, poor growth, high risk behaviors. Further studies demonstrated changes in the epigenetics, neuro, immune, and endocrine biology of toxic stress in children. ACEs accumulate over time, are often inter-generational, and there is a dose dependent link between trauma and symptoms of toxic stress. Burke and colleagues opened the Center for Youth Wellness in 2014 to provide a multidisciplinary team that promotes screening, research, education, and healing from ACEs.
Evidence based treatment to reduce the bio-markers of toxic stress, reduce maladaptive symptoms with a 6 prong approach. A healthy supportive relationship/buffering adult, good sleep, secure nourishment, regular exercise/play, mindfulness, and mental health support (coaching, CBT, ET and others) lower stress hormones and reduced symptoms. With the power of this work, The AAP now has a statement on ACEs, Medi-Cal has plans on screening all children/care givers annually and those under 65yo every 3 years starting in January 2020, and in a few clinics throughout UCSF, ACE screening is directing evidence based care (Matchinger et all, BCH-O).
‘None of us expect to cure a disease by treating its symptoms’ (V. Felitti). Since becoming more versed in ACEs, I feel a shift in my practice. I am certain, like Dr. Felitti, if I had known about ACEs earlier, I would have been a better nurse. I am grateful now to help my patients consider their trauma as a possible driver for maladaptive behaviors and worsening symptoms, help broaden the focus to view these as their best attempts to find a solution. Once that window has been open, patients can imagine and engage in new solutions. The outpatient pediatric specialty AHP group sees many children with chronic disease and increased symptoms and co-morbidities. Knowing that toxic stress disrupts early development of multiple systems and places a high burden on children developing co-morbidities and early death, the AHPs in outpatient specialties have a unique opportunity to act. As pediatric trained providers vested in a longer wellness span and high quality of life in our patients, we are considering piloting ACE screening and referral as a Quality Care True North Pillar effort. We propose piloting a small group of patients (within a few of our practices) to screen for ACE’s and measure before and after integrated support referrals and rate of ED visits.
|
|
|
THE 2019 EXCEPTIONAL ADVANCED HEALTH PRACTITIONER AWARD RECIPIENTS ARE:
Gautham Iyer, NP3
Lead Nurse Practitioner for the Advanced Lung Disease Service
Department of Medicine
Brandon Sessler, PA Sr.
UCSF Orthopedics - Spine Center
Department of Surgery
We received 49 nominations
this year. Thank you to the staff, physicians, AHPs, selection committee members, and patients who contributed to the nomination process.
|
|
EXCEPTIONAL ADVANCED HEALTH PRACTITIONER AWARD NOMINEES 2019
Please assist me in congratulating them all for their professional service.
Alisa Yee NP
Anna Geller, NP
Annika Ehrlich, NP
Caroline Farless, NP
Christine Kim NP
Cynthia Barton, NP
Dorothy Park, CRNA
Elizabeth Rex, NP
Emily Yee, NP
Gabriel Schwartz, NP
Jane Lee, NP
Janice Scudmore, NP
Jennifer Osborn, NP
Julianne Blythe, PA
Libby Wolf, NP
Lorraine Petti, PA
Mary Jane Paras, CRNA
Mathew Somerset, NP
Megan Schoettler, NP
Meredith Russell, NP
Nancy Shepard Lopez, NP
Nicholas Carvelli, NP
Pam Wright, NP
Paula Price, PA
Rebekah Manno, NP
Roseanne Krauter, NP
Ryan Wilson, PA
Samantha Shenoy, NP
Stephanie Jenniches, NP
Stephany Rodriguez, NP
Tara Lacey, PA
Trina Sheedy, PA
Wendy Vining, PA
Willly Ching, CRNA
Yawen Yeh, NP
|
|
|
INFORMED CONSENT MESSAGE FROM ADRIENNE GREEN, MD
|
Colleagues,
During a recent visit to UCSF, The Joint Commission identified opportunities to improve the informed consent process and related documentation. As you already know, physicians have both a legal and ethical duty to make sure that patients fully understand the risks and benefits of any treatment provided to them. This would include AHPs engaged in independent procedures as well. Informed consent is a discussion between a provider and a patient in which all of the risks, benefits and alternatives of treatment are provided to the patient and the patient is given an opportunity to ask questions. This bulletin provides a brief overview of the basic principles of consent and some reminders for documenting the consent process. The UCSF Medical Center policy on informed consent sets forth the hospital's requirements on informed consent discussion and documentation.
Thank you for your ongoing commitment to patient safety at UCSF.
Adrienne Green, MD
Chief Medical Officer, Adult Services
Vice President, Patient Safety and Regulatory Affairs
UCSF Health
|
|
|
|
|
UCSF School of Nursing DNP Program
|
The
UCSF School of Nursing Doctor of Nursing Practice Program is scheduled to have an on-site evaluation by the Commission on Collegiate Nursing Education (CCNE) accreditation team on
September 11 to 13, 2019. As part of the CCNE accreditation process, there is opportunity for the program’s constituents and other interested parties to submit, in writing, comments concerning the program’s qualifications for accreditation that must be received by CCNE no later than
August 21, 2019. All comments must be written in English consistent with CCNE’s policy and should be directed to:
Commission on Collegiate Nursing Education
Attn: Third Party Comments
655 K street NW, Suite 750
Washington, DC, 20001
|
|
|
|
|
April 2019 AHP Open Forum
Next Open Forum: October 24th, 2019.
|
Please Welcome Aletta Gamulo as the Senior Analyst supporting the Office of Advanced Practice. Aletta will oversee programs such as the NP Fellowship, Onboarding Program, the AHP Advisory Board, and its various committees. She came to us several months ago from Transplant Medicine and we are very fortunate to have her analytic skills and other expertise.
Other Highlights: (see link below)
|
|
|
Newly Appointed Nurse Practitioner 3 Cohort
|
Erika Wilson, NP3 Adult Critical Care
Stephany Rodriguez, NP3 Hematology Oncology
Nicholas Carvelli, NP3 Orthopedics
Malia Comstock, NP3 Pediatric Anesthesia
Alisa Yee, NP3 GI Surgical Oncology
|
|
|
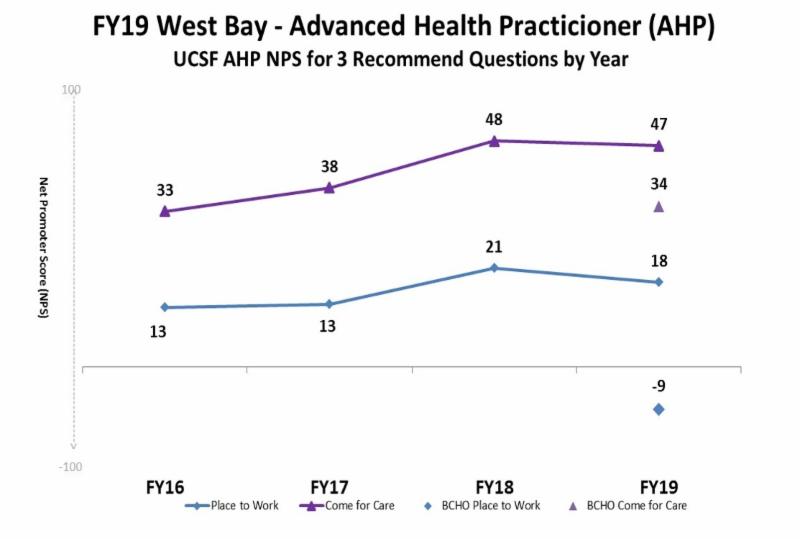
2019 Net Promoter Scores for UCSF Health as a "Place to Work" and "Place to Come for Care"
|
|
|
|
Despite our many advances and improvements, we continue to have more work ahead to create an engaged and supported AHP workforce. For 3 years we had steady improvement of engagement scores but we slipped a little in 2019. The adjacent slide is a high level snapshot of the data for all West Bay AHPs and I will be sharing more detailed information by service soon. I might refer to this as the plateau of my 3 year tenure. You will see the data for BCHO AHPs added for the first time.
|
|
|
Updates regarding Inpatient Documentation and APEX revision to Ambulatory Documentation
|
We are going to pilot a change in the current dot phrase appearance in a couple Pediatric settings first then share the new workflow with all the inpatient settings and finally move to ambulatory last, given we have an ambulatory workflow that generally works. The Office of the President Audit Office is going to scrutinize our utilization of compliant workflows. I ran a report for the month of June 2019 and we had 2436/12559 total AHP encounter types that were not compliant. This is about 19% non-compliance and we need to get to between 5 -10% compliance. Admittedly the report likely has some flaws but I request that every AHP provider please attempt to incorporate the current smart phrase into all encounter types in ambulatory settings. We will start reaching out to providers to remind them to use the smart phrase.
|
|
I wanted to prepare you a change in documentation that will provide greater clarity to coders for independent work and capture all the inpatient work AHPs provide, that remains primarily hidden from view. It is important for AHP providers of care, to document their care visibly. This workflow will resolve hidden clinical care. You will continue to be able to incorporate into your template notes as is current practice. The choices of shared or independent visit types will be clearly identified boxes rather than a drop down. It will also provide an option to choose critical care documentation or not. We have a poor history of capturing billable critical care activity by all providers, which can occur in any clinical location, including ambulatory settings. It will work in any note type and is called a Smart Block.
|
|
|
The UCSF Health Office of Advanced Practice has 15 supported stipends to offset the cost of AHPs presenting at an academic conference in their specialty. Podium/poster/panel presentations will be eligible. Other requirements listed in link below.
|
|
|
 |
Jessica Brennan, NP
Lissa Gray, NP
Ada Edwards, NP
Alisa Yee, NP
Sarah Kabatt, NP
Gabriel Schwartz, NP
Mary Lesh, NP
|
|
|
|
Maura O'Day, NP
Onica Kuch, NP
Claire Parker, NP
JacklinTong, NNP
Annika Erlich, NP
|
|
|
|
Did you know that it is your legal responsibility to ensure the BRN has your most current contact information as a licensee of California. Please update your profile to avoid a fine.
The BRN is moving to an electronic communication strategy with its licensees. The letter to remind you about a license has ended and they are moving to a post card to remind you to update your contact information and will be moving over the next year to an email notification series to remind you to renew your license. This will occur at 90/60/30 days. You will receive no other notifications.
This is a move to reduce paper communication and waste recovery.
|
|
HOW TO UPDATE YOUR CONTACT INFORMATION.
FYI
Follow the instructions they provide, as you do it through the same process as renewing your license but choose the contact information option.
|
|
|
|
Full Circle Story Between Patient and Provider
|
Jason is a post total pancreatectomies with auto-islet cell transplant and is pictured here at his graduation from nursing school. He invited Michelle Klosterman, PNP, RD to do his nurse graduation pinning so it comes full circle that he will now go on to care for his own patients!
Such a great celebration.
Michelle Klosterman and Jason Wong both presented their story to the Monthly Manager's Meeting in June at the request of CEO Mark Laret.
|
|
|
IMPORTANT
Ambulatory AHP Providers ONLY
Please complete the LMS module for this training to be included in the next time study. You will not be included in the dates listed below if you did not complete in the LMS system. Your participation will ready us for the next request from Medi-Cal.
|
The dates are randomly selected and to gain this valuable source of revenue, the time sheets must be completed and returned after signature in blue ink in a timely manner. We must have an 85% participation rate.
|
|
The following training link provides information that ALL ambulatory AHPs must review to be included. ONLY AHP providers that completed the LMS module will receive a link to the TIME SHEET when the next date is announced.
|
|
UCSF HEALTH AHP COMMUNICATIONS COMMITTEE
Our goal is to promote efficient and cohesive communication among AHP's across UCSF Health. AHP's are encouraged to join the "UCSF AHPs" Chatter group in effort to better facilitate sharing of information and connect with other AHPs. Please see the instructions so you don't miss this opportunity to keep up with other AHPs at UCSF Health.
|
|
|
|
AMERICAN HEART ASSOCIATION CERTIFICATION WORKFLOW FOR AHP PROVIDERS RENEWING THEIR BLS, ACLS PALS THROUGH SAFETY TRAINING SEMINARS
They have a list of authorized AHP providers. All others will be denied.
|
|
|
|
|
Schwartz Rounds offer healthcare providers a regularly scheduled time during their fast-paced work lives to openly and honestly discuss the social and emotional issues they face in caring for patients and families. The focus is on the human dimension of patient care. Clinicians and staff have an opportunity to share their experiences, thoughts and feelings on thought-provoking topics drawn from actual patient cases. The premise is that health care providers are better able to make personal connections with patients and colleagues when they have greater insight into their own responses and feelings
|
|
|
The Business of Health Care Depends on Exploiting Doctors and Nurses
One resource seems infinite and free: the professionalism of caregivers.
By
Danielle Ofri
Dr. Ofri practices at Bellevue Hospital in New York.
June 8, 2019
|
|
|
FOR THOSE WITHOUT ACCESS TO NY TIMES
You are at your daughter’s recital and you get a call that your elderly patient’s son needs to talk to you urgently. A colleague has a family emergency and the hospital needs you to work a double shift. Your patient’s M.R.I. isn’t covered and the only option is for you to call the insurance company and argue it out. You’re only allotted 15 minutes for a visit, but your patient’s medical needs require 45. These quandaries are standard issue for doctors and nurses. Luckily, the response is usually standard issue as well: An overwhelming majority do the right thing for their patients, even at a high personal cost. It is true that health care has become corporatized to an almost unrecognizable degree. But it is also true that most clinicians remain committed to the ethics that brought them into the field in the first place. This makes the hospital an inspiring place to work. Increasingly, though, I’ve come to the uncomfortable realization that this ethic that I hold so dear is being cynically manipulated. By now, corporate medicine has milked just about all the “efficiency” it can out of the system. With mergers and streamlining, it has pushed the productivity numbers about as far as they can go. But one resource that seems endless — and free — is the professional ethic of medical staff members. This ethic holds the entire enterprise together. If doctors and nurses clocked out when their paid hours were finished, the effect on patients would be calamitous. Doctors and nurses know this, which is why they don’t shirk. The system knows it, too, and takes advantage. The demands on medical professionals have escalated relentlessly in the past few decades, without a commensurate expansion of time and resources. For starters, patients are sicker these days. The medical complexity per patient — the number and severity of chronic conditions — has steadily increased, meaning that medical encounters are becoming ever more involved. They typically include more illnesses to treat, more medications to administer, more complications to handle — all in the same-length office or hospital visit. By far the biggest culprit of the mushrooming workload is the electronic medical record, or E.M.R. It has burrowed its tentacles into every aspect of the health care system. There are many salutary aspects of the E.M.R., and no one wants to go back to the old days of chasing down lost charts and deciphering inscrutable handwriting. But the data entry is mind-numbing and voluminous. Primary-care doctors spend nearly two hours typing into the E.M.R. for every one hour of direct patient care. Most of us are now putting in hours of additional time each day for the same number of patients. In a factory, if 30 percent more items were suddenly dropped onto an assembly line, the process would grind to a halt. Imagine a plumber or a lawyer doing 30 percent more work without billing for it. But in health care there is a wondrous elasticity — you can keep adding work and magically it all somehow gets done. The nurse won’t take a lunch break if the ward is short of staff members. The doctor will “squeeze in” the extra patients. The E.M.R. is now “conveniently available” to log into from home. Many of my colleagues devote their weekends and evenings to the spillover work. They feel they can’t sign off until they’ve documented all the critical details of their patients’ complex medical histories, followed up on all the test results, sorted out all the medication inconsistencies, and responded to all the calls and messages from patients. This does not even include the hours of compliance modules, annual mandates and administrative requirements that they are expected to complete “between patients.” For most doctors and nurses, it is unthinkable to walk away without completing your work because dropping the ball could endanger your patients. I stop short of accusing the system of drawing up a premeditated business plan to manipulate medical professionalism into free labor. Rather, I see it as a result of administrative creep. One additional task after another is piled onto the clinical staff members, who can’t — and won’t — say no. Patients keep getting their medications and their surgeries and their office visits. From an administrative perspective, all seems to be purring along just fine. But it’s not fine. This month the World Health Organization recognized the serious effects of burnout from chronic workplace stress. Burnout levels among doctors are at new highs, far worse than among the general population, and increasing relentlessly. Burnout among nurses is similarly rising and is highest among those on the front line of patient care. Doctors and nurses commit suicide at higher rates than in almost any other profession. Higher levels of burnout are also associated with more medical errors and compromised patient safety. This status quo is not sustainable — not for medical professionals and not for our patients. Mission statements for health care systems and hospitals are replete with terms like “excellence,” “high-quality” and “commitment.” While these may sound like Madison Avenue buzzwords on a slick brochure, they represent the core values of the people who labor in these institutions. Health care is by no means perfect, but what good exists is because of individuals who strive to do the right thing. It is this very ethic that is being exploited every day to keep the enterprise afloat. The health care system needs to be restructured to reflect the realities of patient care. From 1975 to 2010, the number of health care administrators increased 3,200 percent. There are now roughly 10 administrators for every doctor. If we converted even half of those salary lines to additional nurses and doctors, we might have enough clinical staff members to handle the work. Health care is about taking care of patients, not paperwork. Those at the top need to think about the ramifications of their decisions. Counting on nurses and doctors to suck it up because you know they won’t walk away from their patients is not just bad strategy. It’s bad medicine.
|
|
|
|
GME Grand Rounds - inter-professional opportunity to share experiences.
|
|
|
AHP NEW HIRES COHORT 9 2019
Please welcome these new AHP professionals
|
|
STARTING AHP Cohort 9 for ONBOARDING July 2019
|
|
THEY ARE A GROUP OF NP AND PA PROVIDERS COMING INTO MANY DIFFERENT CLINICAL SPECIALTIES ACROSS THE UCSF HEALTH ENTERPRISE AND OUR AFFILIATE PARTNERS.
|
|
AHP ADVISORY BOARD MINUTES
|
|
|
|
CALIFORNIA HEALTHCARE NEWS
|
A COUPLE ARTICLES RELEVANT TO ADVANCED PRATICE. YOU CAN SUBSCRIBE IF YOU WISH.
|
|
|
|
|
Enhancing Relationship Centered Communication Skills Professional Development for Clinicians
|
|
|
|
|
UCSF HEALTH UPDATES REGARDING TRUE NORTH METRICS
Includes an article on price transparency.
|
|
|
For more information, contact Mitchel Erickson, NP Director of Advanced Practice
|
|
ALL AHP STUDENTS AT UCSF HEALTH FACILITIES
|
All preceptors are required to ensure all students from ALL educational institutions have been vetted by UCSF prior to any educational activities, including employees. UCSF has many parts of the organization involved in this process. Their school needs an affiliation agreement with UCSF, they need health screening to be completed, they require online training for Health and Safety and APEX, and sign a HIPPA form.
New Information to come soon to centralize student engagement at UCSF Health.
|
|
|
WANT TO SHARE YOUR EXPERTISE WITH AHP COLLEAGUES ACROSS THE STATE, THE NATION, OR THE WORLD?
|
|
MORE INFORMATION AND TO BE A PEER SUPPORTER, EMAIL THE FOLLOWING LINK.
Other Resources
:
1.
Mindfulness Mediation
2.
Gratitude Mediation
3.
Loving Kindness Meditation
4.
1-Minute Meditation (for the super-busy)
|
|
|
|
Are you a Clinical Preceptor?
Are you interested in precepting or becoming volunteer clinical faculty?
|
|
|
Presentations, Publications, Recognitions, and News
|
|
|
|
|
|
Pathways to Weight Loss Surgery Clinic Poster Presentation:
Ryan P. Wilson, PA-C, MSPAS, MPH; Elliazar Enriquez, LVN
|
Eli and I are proud to share with you all the exciting news that our Pathways to Weight Loss Surgery Clinic Poster Presentation was chosen as one of the “Top Posters” of the UCSF Health Improvement Symposium for 2019 and Ranked as one of the “Highest Ranked Improvement Initiatives” of the over 210 posters presented this year!
|
|
|
Publication: Ana Marie Torres, NP UCSF Transplant Division
|
“Bi-organ Paired Exchange – Sentinel Case of a Liver-Kidney Swap”
American Journal of Transplantation
|
|
|
American Transplant Congress (ATC) in Boston 2019
UCSF Health AHPs were there representing the UCSF Transplant Program and Advance Health Providers.
Danielle Krieger NP is in a leadership role with the American Society of Transplantation community of practice for advanced practice providers (NPs and PAs). Danielle moderated one of the session at ATC and helped to lead the Transplant Advanced Practice Providers general meeting. Claudia Praglin NP and Eliana Agudelo PA collaborated with Drs. A. Chen and G. Roll in a poster titled “Nodular Regenerative Hyperplasia After Liver Transplant – It is All in the Presentation”. There was time for learning, team bonding, and for planning more projects to continue to represent UCSF Transplant Services and to increase AHP practice and presence at our national meetings.
Pictured also:
Marilyn McEnhill PNP Kidney Transplant and
Giulia Worner NP Pancreas Transplant
|
|
|
|
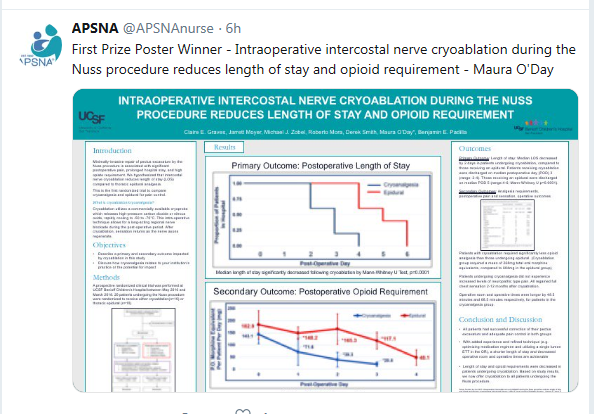
Maura O'Day is a Pediatric Nurse Practitioner in the Pediatric Surgery department and recently presented a poster at the APSNA conference.
Her poster won first place at the APSNA conference.
|
|
|
|
|
Mitchel Erickson, NP with other panelists gave a presentation on - Stakeholder Perspectives on the Value of the Postgraduate Training
at the 2nd Annual Residency and Fellowship Training Consortium Conference , Indianapolis, IN
|
|
|
One Good Thing
Improving the Work Experience at UCSF
Issue 66
Compliments of Diane Sliwka, MD
To make our True North "Our People" efforts more visible at UCSF, this communication provides a highlight of one enhancement, story or tip intended to improve the work experience for clinicians and faculty at UCSF Health.
How To Develop As a Leader
Many physicians find themselves in leadership positions without formal leadership training. Even without formal authority, others are looked to as great leaders. We all want things to work better around us, and if we are going to help make that happen, what can we learn from what great leaders do?
In her book Dare to Lead, Brene Brown defines a leader as:
"Someone who takes responsibility for finding the potential in people and processes, and who has the courage to develop that potential.”
·
Build interpersonal relationships within your group and between otherwise disconnected groups
·
Develop a limitless vision
·
Build relationships with supporters, skeptics and those "on the fence"
·
Surround yourself with diverse people
·
Work on your own Emotional Intelligence (Self Awareness, Empathy, Introspection)
·
Make those who work with you feel valued
Additional Resources:
Thanks to all of you "leaders" who don't throw your hands up when things are hard, but rather see what is possible and work toward that limitless vision. That is one of the things that makes UCSF such an amazing place to work, for me.
Thanks also to Catherine Lucey, whose tweet about leadership inspired this One Good Thing.
|
|
RESOURSE INFORMATION AND LINKS
|
|
|
|
UCSF EMPLOYEE DISCOUNTS AND BENEFITS FOR WORK, LIFE, AND FAMILY
Six Flags - when buying tickets enter promo code UCSF
California Academy of Sciences - when buying tickets for 20% off use promo code UCSF
SF Zoo - use discount code 75001 for $3 off adults, $2 off children with one free train or carousel ride for each ticket
Monterey Bay Aquarium - discount using Store Name UCSF1002
Travel discounts - hotels, packages, cruises. Register for UCSF Passport Discounts, search UCSF Get Away Today
|
|
UPDATING YOUR PAGERBOX CONTACT INFORMATION IS IMPORTANT
In order for other providers to reach you or contact you outside the messaging feature in apex, pagerbox is another mechanism to utilize. This is an internal system and not available to patients. If you do not have a pager, please consider adding your contact information to the pagerbox system. You are only required to respond to pagerbox messages during your normal working hours. All Pagerbox services are now managed by UCSF IT Services.
Feel free to let me know of any problems.
|
|
2018/2019 AHP ADVISORY BOARD
Feel free to reach out to them through global Outlook
|
|
|
Alisa Yee, NP
Willie Ching, CRNA
Shelley Gierat, CRNA
Jeremy Graham, NP
Jennifer Kerney, NP
Laura Kirk, PA - Chair
Maura O’Day, NP
Brandon Sessler, PA
Stacy Wong, NP
Eliana Agudelo, PA
Dana Morgan, PA
|
|
|
|
Laura Weil, CNM
Annette Carley, NP
Gerri Collins Bride, NP
Tracy Curtis, PA
Mitch Erickson, NP
Lissa Gray, NP- Co-chair
Rebekah Kaplan, CNM
Danielle Krieger, NP
Tara Valcarcel, NP
Stacie Rohovit, NP
Michelle Klosterman, NP
|
|
|
|
|
|
Check for any Required Training
|
|
|
THE APEX SMART PHRASE FOR AMBULATORY AND EMERGENCY DEPARTMENT ENCOUNTERS
This phrase MUST be present in ALL encounter notes. ONLY this phrase will work to capture your wRVU attribution. The billing logic was designed for ONLY THIS DOT PHRASE (.ahpvisittype)
|
|
FACE CARDS FOR AHP PROVIDERS
Use the following web-link to complete the ordering process. The instructions are self explanatory. You do not pay but do need to create an account. You may upload a professional photo of your choice or use the RCL or use the RCL photo stock. If you want to use the RCL photo stock. To retrieve a photo taken by RCL, please contact the email below with your name and purpose of use. State for UCSF provider Face Cards.
webservices@ucsfmedctr.org
|
|
Making yourself more visible at UCSF Health
|
|
|
|
In an attempt to ensure all Advanced Health Providers are visible to the public, your patients, and your colleagues at UCSF, please check and to ensure your working title and contact information are correct. Click the link below and complete the log in process and correct what you can. If your title is incorrect then an additional step will be required as this function is controlled by HR. If you find your title needs to be corrected, email me at
mitchel.erickson@ucsf.edu
with your hire title and I will collect information in batches and forward to the correct person. The "Find a Doctor or staff member" portal update is delayed. UCSF Health is building a new web portal and is challenged with migrating data from the old platform to the new platform. Once ready, we will have capacity to add all the AHPs with photos and CV related data. We have been authorized to develop a dedicated AHP Web portal at UCSF Health. More to come.
|
|
|
|
This link will bring you to the UC ME login page. Use the button on the far left at the bottom to access the AHP Resource Manual.
|
This can be completed at the UC Me page by clicking on REQUEST NEW PRIVILEGE.
|
|
|
Look up your credentialed standardized procedures: Must be through VPN or UCSF computer.
Look up all the standardized procedures:
OMAG POLICIES
CIDP
FPPE/OPPE
This link will work from a any computer with/without VPN enabled using IE or Chrome.
Click on Professional Organization Links:
All prescribers of Scheduled Medications will need to register and review upon writing Scheduled Prescriptions
IMPORTANT - RELATED TO YOUR DEA LICENSE
If your DEA license was issued in another state, you need to go online to the DOJ website and change the location to California. Your DEA needs to be in the state where you practice as all state laws are different. YOU
DO NOT
HAVE TO PAY FOR DEA LICENSE OR RENEWAL AS YOU WORK FOR A PUBLIC INSTITUTION.
Very IMPORTANT message from BRN: As of Jan 1st, 2016 if you were licensed in California
prior
to March 1st, 2009 you are required to resubmit fingerprints via the new Live Scan Service. If your renewal seems to be in limbo for unclear reasons, this may be why. After Jan 2018, you will no longer receive a card license. Verification if online only.
This information was extracted directly from State organizations and agencies but does not infer any authority as to its content and you are reminded to check with your state authorities regarding statutes of practice in California.
|
|
Renewal Applications Online
REVISED ANNOUNCEMENT REGARDING RENEWAL APPLICATIONS
Starting January 2017, DEA will no longer send its second renewal notification by mail. Instead, an electronic reminder to renew will be sent to the email address associated with the DEA registration. At this time, DEA will otherwise retain its current policy and procedures with respect to renewal and reinstatement of registration. This policy is as follows: If a renewal application is submitted in a timely manner prior to expiration, the registrant may continue operations, authorized by the registration, beyond the expiration date until final action is taken on the application.
DEA allows the reinstatement of an expired registration for one calendar month after the expiration date. If the registration is not renewed within that calendar month, an application for a new DEA registration will be required. Regardless of whether a registration is reinstated within the calendar month after expiration, federal law prohibits the handling of controlled substances or List 1 chemicals for any period of time under an expired registration.
|
|
If you have any suggestions regarding content or additions to the monthly newsletter, please send them to: (submission deadline is 1st of each month)
|
|
|
|
|
|
|